Stroke (Cerebrovascular Accident)
Key Points
- “Time is brain” — brain cells die within minutes without oxygen; early recognition and intervention are critical
- 87% of strokes are ischemic (clot occlusion); 13% are hemorrhagic (vessel rupture)
- BEFAST: Balance, Eyes, Face, Arm, Speech, Time — standardized stroke recognition mnemonic
- tPA (alteplase): Only FDA-approved for ischemic stroke; must be given within 3 hours (up to 4.5 hours select patients)
- First diagnostic test: Non-contrast CT scan — rules out hemorrhage before tPA can be given
- TIA: “Mini-stroke” — same symptoms but resolves without permanent damage; 18% stroke risk within 90 days
- Telemedicine-supported monitoring and urgent video NIHSS assessment can accelerate stroke-team activation, but definitive acute treatment still requires immediate in-person emergency care.
Pathophysiology
A stroke (cerebrovascular accident, CVA) is a sudden interruption of blood flow to the brain causing irreversible neuronal death if not treated rapidly. The brain receives roughly 15 to 20 percent of resting cardiac output, and focal perfusion loss can cause irreversible tissue injury within minutes. Over 800,000 strokes occur annually in the US; nearly 75% occur in adults over age 65. Stroke remains the fifth-leading cause of death and a leading cause of long-term disability in the United States.
Cerebral Perfusion Context
The circle of Willis is an arterial collateral network that helps preserve cerebral perfusion when one vascular segment is narrowed or occluded. Collateral support can reduce infarct severity in selected flow-limiting lesions.
- Anterior circulation: Internal carotid pathways supplying most of the cerebrum (frontal, parietal, lateral temporal, and anterior deep-hemisphere regions).
- Posterior circulation: Vertebral arteries join to form the basilar artery and supply the brainstem, cerebellum, occipital lobes, and part of the deep hemisphere (including thalamic regions).
Ischemic Stroke (87%)
Mechanism: Occlusion of a cerebral artery → loss of perfusion → neuronal death.
| Type | Mechanism | Risk Factors |
|---|---|---|
| Thrombotic | Plaque (atherosclerosis) → thrombus forms in cerebral vessel | Hypertension, atherosclerosis |
| Embolic | Clot forms elsewhere (heart, carotid), travels to brain | Atrial fibrillation (most common cardiac source), valvular disease |
| Lacunar | Small vessel occlusion in penetrating arteries | Hypertension, diabetes, high cholesterol |
| Cryptogenic | Cause undetermined; higher incidence in African Americans and Hispanics | — |
TIA (Transient Ischemic Attack): Temporary occlusion with transient stroke-like symptoms and no persistent infarction evidence; episodes often resolve within minutes and commonly within about 1 hour. Considered a warning sign of imminent stroke: 90-day stroke risk after TIA is ~18%.
Typical presentation differences:
- Ischemic thrombotic: Symptoms may evolve gradually or fluctuate before stabilizing.
- Ischemic embolic: More abrupt onset with severe deficits often present early.
- Hemorrhagic: Abrupt presentation with severe headache, neck pain, photophobia, nausea/vomiting, and higher early depressed-consciousness risk.
Hemorrhagic Stroke (13%)
Mechanism: Rupture of a cerebral vessel → blood accumulates → increased intracranial pressure (ICP) → brain compression and ischemia.
| Type | Location | Common Cause |
|---|---|---|
| Intracerebral hemorrhage (ICH) | Within brain tissue | Hypertension (most common), anticoagulants |
| Subarachnoid hemorrhage (SAH) | Subarachnoid space (around brain) | Ruptured aneurysm, AVM rupture |
SAH hallmark: Sudden “worst headache of my life” — thunderclap onset, often with nausea, vomiting, photophobia, nuchal rigidity.
Clinical Manifestations
BEFAST Mnemonic (Stroke Recognition)
| Letter | Assessment | Signs |
|---|---|---|
| B — Balance | Sudden loss of balance or coordination | Ataxia, falls |
| E — Eyes | Sudden vision loss or change | Hemianopia, diplopia |
| F — Face | Facial asymmetry | Facial drooping on one side |
| A — Arm | Arm weakness or drift | Hemiparesis/hemiplegia |
| S — Speech | Slurred or confused speech | Dysarthria, aphasia |
| T — Time | Time to call 911 immediately | Document “last known well” time |
FAST-only screening can miss some posterior-circulation strokes; BEFAST improves detection by adding balance and visual-change cues.
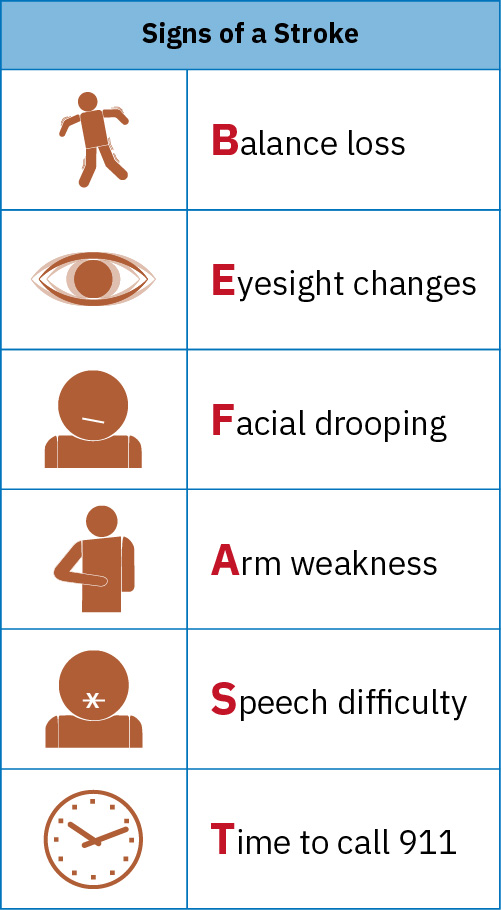 Illustration reference: OpenStax Clinical Nursing Skills Ch.15.
Illustration reference: OpenStax Clinical Nursing Skills Ch.15.
Additional Symptoms by Stroke Location
- Right hemisphere: Visual/spatial deficits, impulsivity, personality changes, left-sided deficits
- Left hemisphere: Speech and language deficits (aphasia), analytic thinking impairment, right-sided deficits
- Mimic caution: Peripheral facial palsy patterns (for example Bell palsy) may resemble stroke at presentation; sudden focal deficits should still be treated as stroke until urgent workup excludes cerebrovascular cause.
Common Deficits by Vessel Territory
- MCA: Hemiparesis/hemiplegia, aphasia, homonymous hemianopsia.
- ICA: Contralateral face-arm-leg sensory/motor deficits, aphasia/apraxia, hemianopsia, possible unilateral neglect.
- ACA: Contralateral leg-predominant weakness/sensory loss, gait impairment, cognitive or affective change, urinary incontinence.
- VA/PICA: Dizziness, nystagmus, dysphagia, dysarthria, ataxia/vertigo, crossed sensory findings.
- Basilar artery: Quadriplegia, bulbar weakness, or locked-in syndrome in severe infarction.
- PCA: Visual deficits, memory impairment, pupillary abnormalities, and sensory deficits.
Complications of CVA
Hemiparesis/hemiplegia, dysphagia, aphasia, dysarthria, homonymous hemianopsia, bladder incontinence, seizures (first 24 hours), emotional lability, aspiration risk.
Assessment and Diagnostics
Neurological Assessment Tools:
- NIHSS (NIH Stroke Scale): Standardized severity rating (0 to 42); higher score = more dysfunction and poorer expected outcome
- Glasgow Coma Scale (GCS): Level of consciousness assessment
- “Last known well” time: Most critical question — determines tPA eligibility window
- NIHSS-linked highly predictive acute findings include facial droop, arm weakness/drift, and speech abnormality.
- In remote pathways, structured video-guided NIHSS tasks can support early cue recognition while EMS transport is being activated.
Rapid stroke-pathway activation should include immediate transport to an accredited stroke center or activation of in-hospital stroke-team protocol. Many stroke-ready pathways target CT initiation within about 25 minutes of arrival with imaging interpretation within about 45 minutes.
Diagnostic Tests:
| Test | Purpose |
|---|---|
| CT scan (non-contrast) | First-line — rules out hemorrhage before tPA administration |
| CT with contrast/CT perfusion | Defines infarct location/size and penumbra (salvageable marginal-flow tissue) in selected pathways |
| MRI | Brain lesions, extent of infarction |
| Carotid Doppler ultrasound | Assesses carotid artery occlusion |
| Cardiac echocardiogram | Evaluates for cardiac embolic source (A-fib) |
| Cerebral angiogram | Identifies arterial occlusion and selected hemorrhagic-source vascular abnormalities |
| PT, INR, aPTT | Baseline coagulation before fibrinolytic/anticoagulant therapy |
Signs of Increased Intracranial Pressure (ICP)
Increased ICP — Priority Assessment
Hemorrhagic stroke patients are at highest risk for ICP elevation within the first 72 hours.
- Earliest sign: Decreased level of consciousness
- Restlessness, agitation, confusion
- Headache, nausea/vomiting
- Seizures (especially first 24 hours)
- Severe hypertension + bradycardia (Cushing’s triad)
- Late signs: Decerebrate (extension) or decorticate (flexion) posturing
Medical Management
Ischemic Stroke — tPA (Alteplase)
tPA Administration — Time-Critical
IV alteplase (tPA) must be administered within 3 hours of stroke onset (up to 4.5 hours in select patients).
Contraindications to tPA:
- Age over 80 years
- Current anticoagulant use
- History of both stroke and diabetes
- Recent surgery or head trauma
Post-tPA: Do NOT give aspirin or anticoagulants within 24 hours of tPA.
Ongoing therapy: Aspirin 24–48 hours after onset (if tPA not used or after 24-hour waiting period); anticoagulants for A-fib-related strokes.
Endovascular therapy: Mechanical thrombectomy for large vessel occlusion — extends treatment window.
Hemorrhagic Stroke Management
- Blood pressure control: Gradual reduction to 150/90 mmHg — beta-blockers, ACE inhibitors, calcium channel blockers, or hydralazine
- Surgical intervention: For cerebellar hemorrhage >3 cm, hydrocephalus, brain stem compression
- Aneurysm/AVM: Neurosurgical clipping or coiling to stop bleeding
- Vasospasm management context: Nimodipine may be used after subarachnoid hemorrhage in selected care pathways.
Nursing Interventions (Acute Phase)
Priority Assessments:
- Neurological checks: LOC, Glasgow Coma Scale, pupillary response, motor strength
- Airway patency, respiratory status
- Vital signs — frequent monitoring
- Cardiac rhythm monitoring (detect A-fib)
- Blood glucose trending because dysglycemia can worsen neurologic injury
- Seizure monitoring (especially first 24 hours)
- Swallowing assessment — aspiration precautions
- Sodium and intake/output trending for potential SIADH-associated fluid/electrolyte shifts
Key Nursing Interventions:
- Maintain HOB elevation 30° to reduce ICP
- Aspiration precautions (dysphagia risk): NPO until swallowing assessment completed
- Skin integrity — frequent repositioning for immobile patients
- Fall prevention — hemiparesis/hemiplegia and confusion increase risk
- Communication support — provide alternative communication strategies for aphasia
- Follow DVT prophylaxis and constipation-prevention plans (including stool-softener protocols when ordered)
- Avoid lifting or pulling on a flaccid/affected arm; protect affected extremities from dependent edema and injury
- Apply visual-field compensation strategies (approach from intact side and cue scanning toward affected field)
- Assess homonymous-hemianopsia impact on eating, hygiene, and community mobility; reinforce active head-turn scanning and postpone driving until formal visual/cognitive clearance.
- If receiving alteplase/anticoagulants, implement strict bleeding precautions
ICP-Focused Stroke Care
- Keep neck midline and avoid sudden neck/hip flexion that can increase intrathoracic pressure and ICP.
- Avoid clustering high-stimulation activities; use low-stimulus pacing to reduce ICP spikes.
- Provide oxygenation support and hyperoxygenate around suctioning when indicated.
- Use sedatives cautiously because they can mask neurologic changes.
Rehabilitation Goals: Interdisciplinary team (PT, OT, speech therapy, case management):
- Improved mobility and self-care
- Dysphagia management and aspiration prevention
- Communication optimization (speech therapy for aphasia/dysarthria)
- Emotional support for lability, coping, and depression
Health Teaching and Secondary Prevention
- Reinforce recurrent-stroke prevention: smoking cessation, blood-pressure and glucose control, lipid reduction, physical activity, diet improvement, and adherence to prescribed medications.
- Include individualized risk-counseling context, noting sex- and population-level disparities (for example women and selected American Indian/Alaska Native communities) when planning prevention follow-up.
- Teach client/caregiver stroke-warning recognition (BEFAST) and immediate emergency activation for recurrent symptoms.
- In telemedicine-enabled home monitoring plans, teach patients to treat new unilateral weakness, facial droop, or speech changes as emergency cues and activate EMS first.
- If discharged on anticoagulants, teach bleeding-risk surveillance and urgent reporting triggers.
- Teach safe use of assistive devices to reduce fall risk during recovery.
Related Concepts
- neurological-system — Cerebrovascular anatomy
- ischemic-stroke-acute-treatment-and-secondary-prevention — Detailed reperfusion windows, contraindication screening, and postacute prevention pathway.
- hemorrhagic-stroke-acute-management-and-icp-control — Bleed-source control, ICP-focused stabilization, and neurosurgical escalation pathway.
- common-neurological-disorders-recognition-and-priority-care — Neurological assessment frameworks
- anticoagulants — Prevention of embolic recurrence; contraindicated during acute phase
- antihypertensives — Hypertension management as primary risk factor
- hypertension-assessment-and-management — Hemorrhagic stroke prevention
- cardiovascular-system — Atrial fibrillation as embolic source
- fall-prevention — Post-stroke fall risk management
Self-Check
- A patient arrives at the ED with sudden right-sided arm weakness and speech difficulty, “last known well” 2 hours ago. CT scan is negative for hemorrhage. What medication may be administered, and what is the time-critical consideration?
- A patient with hemorrhagic stroke who was neurologically stable suddenly becomes lethargic with bradycardia and severe hypertension. What complication do these findings suggest, and what is the priority intervention?
- A nurse is assessing a post-stroke patient and notes they are coughing during mealtime. What complication is the patient at risk for, and what nursing action is most appropriate?