Antihypertensives
Key Points
- Six major classes: ACE inhibitors, ARBs, beta-blockers, calcium channel blockers, thiazide diuretics, and direct vasodilators
- ACE inhibitors: Hallmark adverse effect is persistent dry cough; both ACE inhibitors and ARBs are contraindicated in pregnancy (fetal harm/death — Boxed Warning)
- Beta-blockers: Hold if apical HR <60 bpm; NEVER stop abruptly — taper over 1–2 weeks
- Angioedema from ACE inhibitors = life-threatening emergency — stop drug immediately
- Patients commonly take multiple antihypertensives that work synergistically on different mechanisms
Drug Class Overview
Antihypertensives are medications that lower elevated blood pressure. Hypertension is a major risk factor for myocardial infarction, stroke, heart failure, and renal disease. Multiple classes target different points in blood pressure regulation — most patients with Stage 2 hypertension (≥140/90 mm Hg) require combination therapy with complementary mechanisms.
Major Classes
ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors)
Mechanism: Block conversion of Angiotensin I → Angiotensin II in the RAAS system → vasodilation + reduced aldosterone release → decreased sodium/water retention.
Examples: Captopril, lisinopril, enalapril, ramipril, benazepril (suffix: “-pril”).
Indications: Hypertension, heart failure, diabetic nephropathy (slow progression), post-myocardial infarction.
Adverse Effects:
- Persistent dry cough (most common, 10–15% of patients; due to bradykinin accumulation) — if intolerable, switch to ARB
- Hyperkalemia — avoid potassium supplements and salt substitutes
- Angioedema (rare but life-threatening) — facial/tongue swelling, difficulty breathing → STOP drug, call 911, epinephrine ready
- Hypotension (especially first dose), proteinuria
ACE Inhibitor Pregnancy Contraindication — Boxed Warning
ACE inhibitors cause fetal renal damage and fetal/neonatal death when administered in the 2nd and 3rd trimesters. Discontinue immediately if patient becomes pregnant. Counsel all women of childbearing age.
ARBs (Angiotensin II Receptor Blockers)
Mechanism: Block Angiotensin II receptors → vasodilation and reduced aldosterone → similar effect to ACE inhibitors but without bradykinin accumulation.
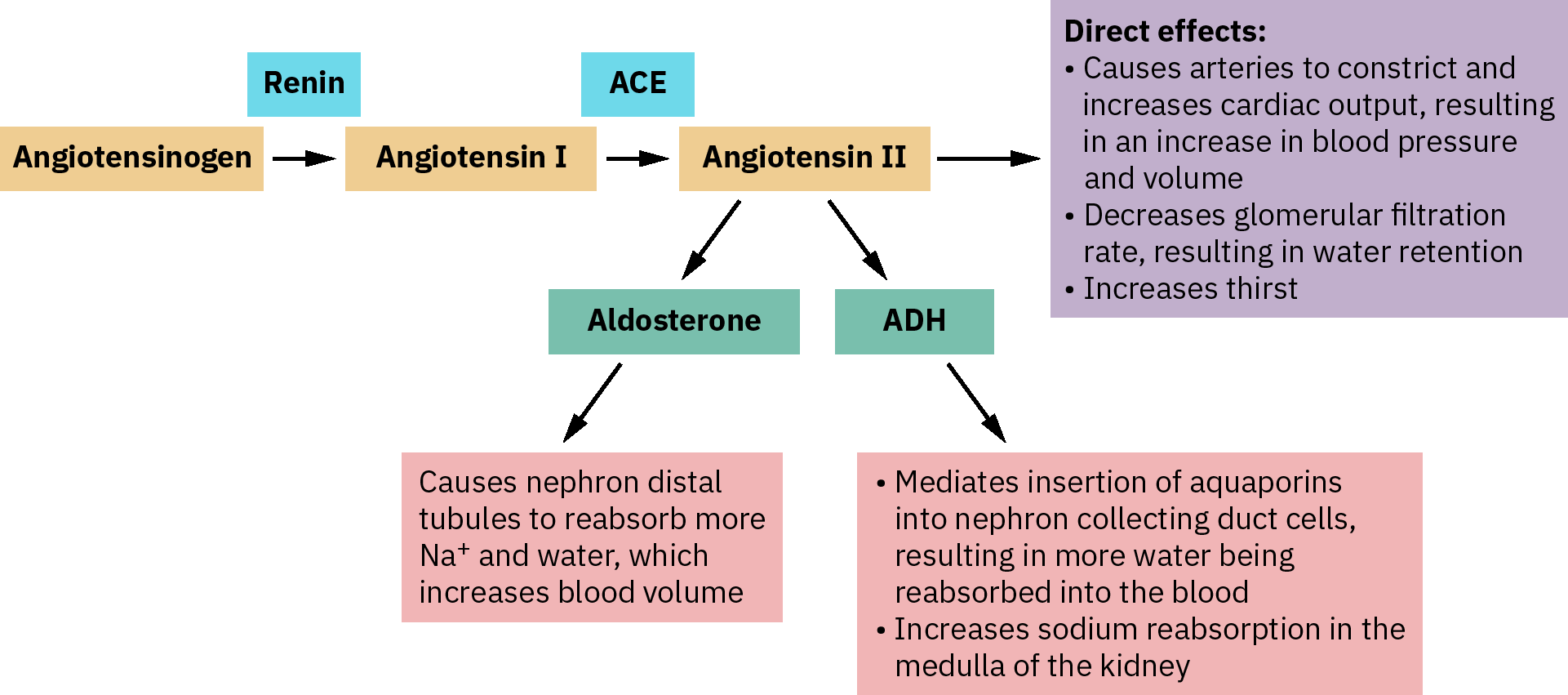 Illustration reference: OpenStax Pharmacology Ch.19.2.
Illustration reference: OpenStax Pharmacology Ch.19.2.
Examples: Losartan, valsartan, irbesartan, olmesartan (suffix: “-sartan”).
Key Difference from ACE Inhibitors: ARBs do NOT cause the persistent cough — preferred for ACE inhibitor-intolerant patients.
Adverse Effects: Hypotension, dizziness, hyperkalemia, angioedema (less common than ACE inhibitors), proteinuria.
Boxed Warning: Contraindicated in pregnancy — same risk as ACE inhibitors.
ARB + ACE Inhibitor Combination
Combining ACE inhibitors and ARBs increases risk of hypotension, hyperkalemia, and renal impairment without additional blood pressure benefit. Generally avoid dual RAAS blockade.
Beta-Blockers (Beta-1 Selective Antagonists)
Mechanism: Block beta-1 adrenergic receptors in the heart → decreased heart rate and contractility → decreased cardiac output and blood pressure.
Examples: Metoprolol (selective beta-1), atenolol, bisoprolol; carvedilol (non-selective beta-1/beta-2/alpha).
Indications: Hypertension, heart failure, post-MI, atrial fibrillation (rate control), angina.
Key Nursing Points:
- Check apical pulse before administration — hold and notify provider if HR <60 bpm (unless alternate parameters specified)
- Do NOT crush extended-release (ER) formulations (metoprolol succinate)
- Monitor blood glucose in diabetics: Beta-blockers mask tachycardia (key sign of hypoglycemia); glycemic control monitoring essential
- NEVER stop abruptly: Taper over 1–2 weeks — abrupt discontinuation → rebound hypertension, chest pain, or MI
Adverse Effects: Bradycardia, fatigue, depression, insomnia, erectile dysfunction, cold extremities, bronchoconstriction (at high doses or non-selective agents — use caution in asthma/COPD).
Calcium Channel Blockers (CCBs)
Mechanism: Block calcium channels in vascular smooth muscle and cardiac tissue → smooth muscle relaxation → vasodilation → decreased BP and decreased cardiac workload.
Examples:
- Dihydropyridines (primarily vascular; preferred for HTN): Amlodipine, nifedipine, felodipine
- Non-dihydropyridines (cardiac + vascular; also used for arrhythmias): Verapamil, diltiazem
Adverse Effects: Peripheral edema (especially dihydropyridines), headache, flushing, reflex tachycardia (nifedipine). Verapamil → constipation, bradycardia.
Interaction: Verapamil and diltiazem inhibit CYP3A4 → increased levels of many drugs including statins, macrolides.
Thiazide Diuretics — See diuretics
Hydrochlorothiazide (HCTZ) is a first-line antihypertensive (see diuretics.md for details). Frequently combined with ACE inhibitors or ARBs. Key risk: hypokalemia.
Direct Vasodilators
Hydralazine: Direct relaxation of arterial smooth muscle → vasodilation.
Indications: Hypertension (severe/refractory), hypertensive emergency in pregnancy (eclampsia), and selected symptomatic heart-failure pathways in combination with isosorbide dinitrate.
In heart-failure adjunct use (hydralazine/isosorbide dinitrate), this combination is often considered after first-line optimization, with strongest mortality evidence in self-identified Black HFrEF populations and possible adjunct benefit when first-line pathways are not tolerated. For acute symptomatic hypertensive events, inpatient protocols may use IV hydralazine and IV beta-blocker pathways with serial BP/rhythm telemetry plus target-organ injury labs.
Nursing Considerations: Use cautiously in clients with coronary artery disease, rheumatic mitral-valve disease, or prior cerebrovascular accidents; in pregnancy, use only when expected benefit outweighs fetal risk. For hydralazine/nitrate combinations, reassess hypotension risk carefully and avoid PDE5-inhibitor overlap because profound blood-pressure collapse can occur.
Adverse Effects: Drug-induced systemic lupus erythematosus (SLE) — butterfly facial rash, joint pain, fever. Monitor CBC and antinuclear antibody (ANA) titers. Orthostatic hypotension, palpitations, angina, tremor, paresthesia, headache, nausea, vomiting, and diarrhea.
Alpha-2 Agonists
Clonidine: Stimulates central alpha-2 receptors → decreased sympathetic outflow → vasodilation and decreased peripheral resistance.
Adverse Effects: Sedation, dry mouth/dry eyes, bradycardia, orthostatic hypotension.
Critical: Do NOT stop abruptly → rebound hypertension (potentially severe).
Nursing Assessment
Before Administration:
- Obtain BP and apical HR — compare to parameters; hold for BP <90/60 or HR <60 (unless other orders)
- Review current medications for interactions (especially potassium with ACE inhibitors/ARBs)
- If ACE inhibitors are combined with lithium, monitor closely for rising lithium levels and toxicity symptoms
- Assess for pregnancy (ACE inhibitors and ARBs: teratogenic)
- Review renal function (many antihypertensives affect renal clearance)
Ongoing Monitoring:
- BP trend (lying, sitting, standing for orthostatic hypotension)
- Serum potassium — hyperkalemia risk with ACE inhibitors, ARBs, potassium-sparing diuretics
- Peripheral edema — especially with CCBs
- Angioedema: swelling of face, lips, tongue, throat → emergency response
- Persistent cough → report; may require switch from ACE inhibitor to ARB
- In acute severe presentations, trend neurologic/cardiopulmonary symptoms alongside serial blood-pressure measurements and target-organ testing.
Patient Education:
- Take at the same time each day; never skip or double dose
- Rise slowly from bed/chair to prevent orthostatic dizziness
- Beta-blockers: never stop without tapering under provider guidance
- ACE inhibitors/ARBs: avoid salt substitutes (contain potassium) and NSAIDs (decrease effectiveness, increase renal risk)
- Clonidine patch: apply to hairless skin; rotate sites; never stop abruptly
- Clonidine users should avoid alcohol and other CNS depressants and report troublesome dry eyes/mouth
- Hydralazine users should call the care team for infection symptoms, lupus-like rash/joint pain, or if two or more doses are missed
- Monitor home BP and maintain medication log
Related Concepts
- hypertension-assessment-and-management — Clinical management of hypertension
- heart-failure — ACE inhibitors, ARBs, beta-blockers are cornerstone heart failure therapy
- diuretics — Thiazide diuretics as antihypertensive class
- coronary-artery-disease — Beta-blockers and CCBs for angina and post-MI management
- potassium-balance-disorders — Hyperkalemia risk with ACE inhibitors and ARBs
- kidney-disease — ACE inhibitors and ARBs protect kidneys in CKD/diabetes
Self-Check
- A patient on lisinopril develops a persistent dry cough. What alternative drug class provides similar mechanism but without the cough?
- Before administering metoprolol, the patient’s apical heart rate is 54 bpm. What is the nurse’s priority action?
- A patient on an ACE inhibitor reports sudden swelling of the lips and difficulty swallowing. What is this reaction, and what is the immediate nursing response?