Hypertension Assessment and Management
Key Points
- Normal adult blood pressure is less than 120/80 mm Hg, and hypertension is chronic elevation above this level.
- Hypertension is often asymptomatic and commonly identified through repeated elevated readings over time.
- Elevated-range blood pressure requires closer follow-up because progression risk to stage-based hypertension is increased.
- Primary hypertension has no single identifiable cause, while secondary hypertension is linked to medical conditions or medications.
- Hypertensive crisis is defined as blood pressure greater than 180/120 mm Hg and requires urgent clinical escalation.
- Nonmodifiable risk factors include age, family/genetic burden, sex, and race/ethnicity patterns; modifiable factors include diabetes, high-sodium diet, low potassium intake, inactivity, obesity, tobacco, and excess alcohol use.
- Neurohormonal regulation through the renin-angiotensin-aldosterone system and vasopressin can increase blood pressure through vasoconstriction and fluid retention.
- Uncontrolled hypertension increases risk for major complications including myocardial infarction, heart failure, stroke, peripheral arterial disease, aneurysm, vision loss, and kidney damage.
- Core management combines lifestyle modification, antihypertensive medication adherence, and consistent home blood pressure monitoring.
- Dietary patterns such as DASH and Mediterranean-style eating reduce blood-pressure burden by lowering sodium and unhealthy-fat intake while improving nutrient quality.
- DASH-style teaching prioritizes lower sodium/saturated/trans fat intake with higher potassium, calcium, magnesium, fiber, and protein intake, alongside activity and healthy-weight goals.
Pathophysiology
Hypertension reflects sustained elevation in arterial pressure that increases cardiac workload and vascular stress over time. Progressive pressure-related injury can affect multiple organs, especially the heart, brain, kidneys, and retinal vessels.
Vascular remodeling and stiffening often progress in parallel with pressure elevation. Arteriosclerotic stiffness and atherosclerotic plaque narrowing can both raise intravascular pressure, while uncontrolled hypertension further accelerates vessel-wall injury and plaque-related complications.
Most adults have primary hypertension, which develops gradually and is associated with multifactorial influences including age, family history, race, diet, stress, and physical inactivity. Secondary hypertension occurs when elevated pressure is driven by an identifiable condition or medication effect.
Neurohormonal pathways further modulate pressure burden. RAAS activation increases angiotensin II-mediated vasoconstriction and aldosterone-driven sodium and water retention, while vasopressin increases water reabsorption and vasoconstrictive tone, together raising blood pressure when compensatory responses are sustained.
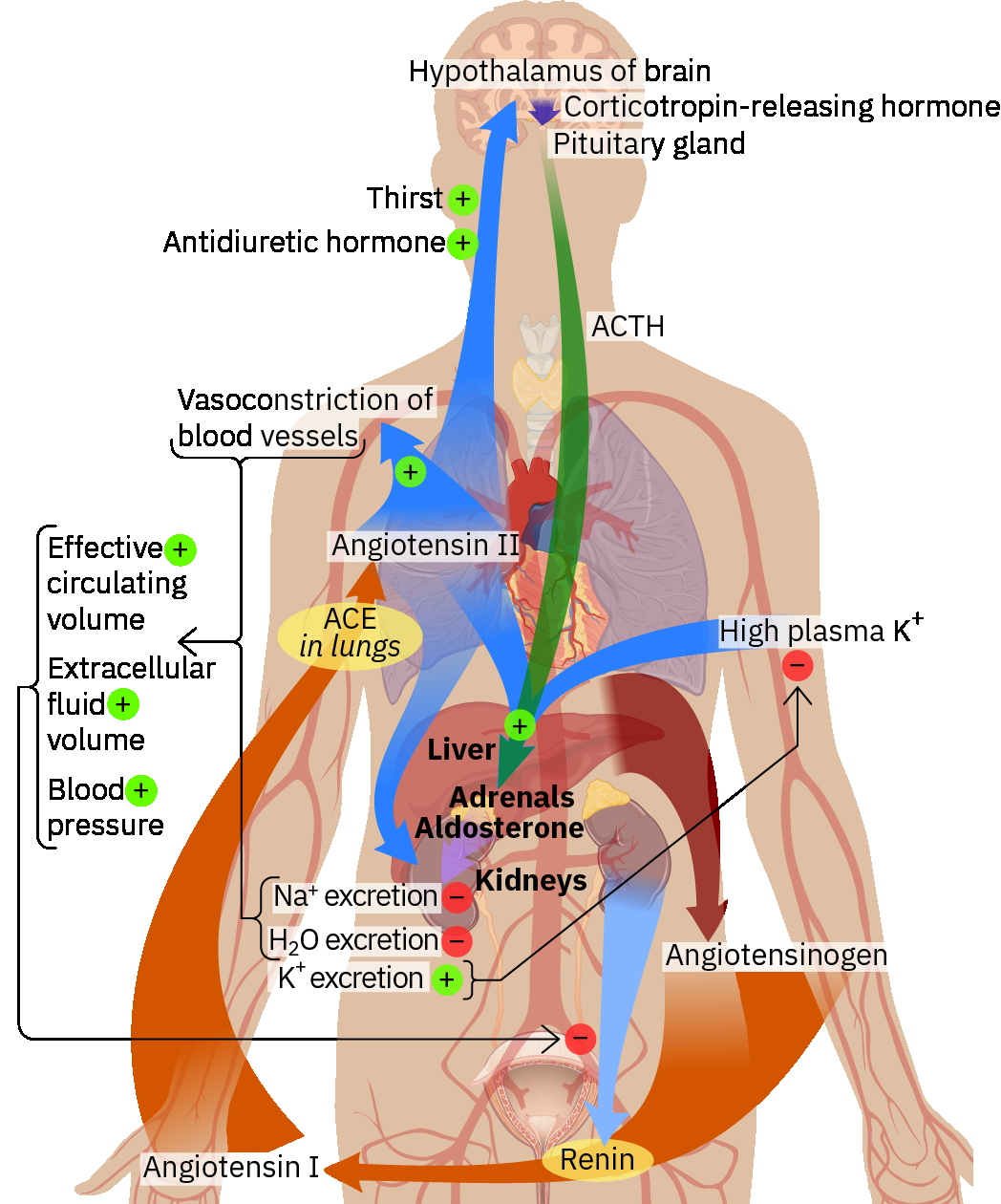 Illustration reference: OpenStax Pharmacology Ch.18.1.
Illustration reference: OpenStax Pharmacology Ch.18.1.
Diet quality is a major modifiable driver of long-term pressure burden. Patterns high in highly processed foods, sodium, added sugars, and saturated or trans fats worsen vascular risk, while patterns emphasizing unsaturated fats, plant-forward proteins, and minimally processed foods support blood-pressure and cardiovascular risk reduction.
Although this note primarily addresses adults, hypertension also affects pediatric populations and requires age-appropriate screening and prevention counseling in family-centered care settings.
Classification
- Normal: Systolic less than 120 and diastolic less than 80 mm Hg.
- Elevated: Systolic 120-129 and diastolic less than 80 mm Hg.
- Hypertension Stage 1: Systolic 130-139 or diastolic 80-89 mm Hg.
- Hypertension Stage 2: Systolic 140 or higher or diastolic 90 or higher mm Hg.
- Hypertensive Crisis: Systolic higher than 180 or diastolic higher than 120 mm Hg.
- Urgency versus emergency distinction: Severe symptomatic elevation without target-organ injury is urgency; similar elevation with target-organ injury (for example pulmonary edema or kidney failure) is emergency and requires immediate escalation.
Nursing Assessment
NCLEX Focus
Prioritize confirmation of persistent elevation, end-organ risk screening, and teaching for self-monitoring.
- Assess for elevated blood pressure trends, noting many clients remain asymptomatic until screening detects abnormal readings.
- Reinforce routine annual screening and increase measurement frequency when elevated trends begin.
- Assess for associated symptoms when present, such as headache, epistaxis, fatigue, nausea, chest pain, dyspnea, blurred vision, dizziness, or fainting.
- Confirm blood pressure using proper technique, with readings in both arms while the client is seated and relaxed.
- Confirm diagnosis trend with readings from at least two separate clinic occasions (commonly spaced by about two weeks) and review serial home/community logs when available.
- Use premeasurement controls to reduce false elevation: properly sized cuff, legs uncrossed, back/arm support, and avoidance of smoking/eating for at least about 30-45 minutes before measurement when feasible.
- If automated measurement is elevated, follow with a manual reading when feasible to validate the result.
- Review home blood pressure logs across multiple dates and times to support diagnosis and treatment planning.
- Review diagnostic workup results (for example 12-lead ECG, basic metabolic panel, lipid profile, fasting glucose, and urine protein) to identify contributors and early end-organ effects.
- Track anthropometric risk markers with blood-pressure trends, including BMI pattern and central-adiposity screening with waist circumference.
- Assess social-determinant barriers that delay hypertension detection or treatment (for example transportation reliability, clinic-hour access, cost barriers, or reduced primary-care continuity).
- Monitor for signs of target-organ effects and review diagnostic findings such as echocardiography, fundoscopic exam findings, serum creatinine, and estimated GFR.
Nursing Interventions
- Teach home blood pressure technique and reinforce consistent logging for follow-up visits.
- Provide lifestyle counseling on low-sodium dietary patterns, regular aerobic activity, weight management, alcohol moderation, and smoking cessation.
- In alcohol-risk education, explain that heavy daily intake can raise blood-pressure burden and long-term cardiomyopathy/CAD risk (commonly women >4 drinks/day and men >5 drinks/day are high-risk patterns).
- Set activity goals toward at least about 150 minutes/week of moderate aerobic activity unless contraindicated.
- Teach condition-specific food-pattern options such as DASH and Mediterranean-style eating, emphasizing limited processed foods, saturated/trans fats, added sugars, and sodium.
- Reinforce fat-quality and protein-food substitutions (for example olive-oil and nut/seed patterns, legumes and other plant proteins, and lean-meat choices when meat is consumed).
- For DASH counseling, emphasize foods rich in potassium, calcium, magnesium, fiber, and protein while coordinating diet teaching with physical-activity and weight-management plans.
- Use individualized sodium targets in teaching: most prevention plans start near 2,300 mg/day, with tighter limits used in selected high-risk clients when tolerated.
- Counsel on reducing or eliminating caffeine when readings are labile or recurrently elevated.
- Reinforce stress-management strategies such as paced breathing, progressive muscle relaxation, and healthy coping plans.
- Administer antihypertensive therapy safely, monitor therapeutic response, and teach side-effect reporting.
- Promote medication adherence and instruct clients to avoid independent medication changes without provider guidance.
- Coordinate follow-up pathways that fit access barriers (for example flexible scheduling, home BP-log review plans, community resource linkage).
- Teach clients to promptly report reduced perfusion symptoms (for example severe headache, dizziness, syncope, chest pain, or new neurologic deficits) and review escalation steps.
- Escalate rapidly for severe symptomatic readings even before classic crisis thresholds when presentation suggests evolving end-organ risk.
- In acute symptomatic presentations, prepare for provider-directed inpatient pathways such as IV antihypertensives, target-organ laboratory evaluation, and telemetry-based serial BP/rhythm monitoring.
- Use SMART goal framing with patient preferences; common measurable outcomes include movement toward <120/80 mm Hg, medication adherence, and sustained risk-factor modification.
- Evaluate outcomes at each intervention cycle and after new diagnostic/laboratory data; revise the care plan if blood-pressure goals are only partially met or not met.
Silent Progression Risk
Hypertension may progress without symptoms while causing cumulative end-organ damage; ongoing monitoring and follow-up are safety-critical.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| diuretics | class-based agents | Reduce sodium and fluid load; monitor blood pressure response trends. |
| beta-blockers | class-based agents | Lower heart rate and cardiac workload; monitor tolerance and pulse. |
| ace-inhibitors | class-based agents | Reduce angiotensin II formation; reinforce adherence and monitoring. |
| angiotensin-ii-receptor-blockers | class-based agents | Block angiotensin II effects; monitor blood pressure effect. |
| calcium-channel-blockers | class-based agents | Promote vasodilation; evaluate therapeutic response and tolerance. |
| antihypertensives (alpha-agonists) | class-based agents | Support blood pressure reduction; teach safe, scheduled use. |
| antihypertensives (direct-vasodilators) | class-based agents | Decrease vascular tone; monitor for blood pressure changes. |
Clinical Judgment Application
Clinical Scenario
A middle-aged client reports no symptoms but presents with repeated clinic and home readings in the Stage 1 to Stage 2 range and inconsistent medication use.
- Recognize Cues: Persistent elevated systolic and diastolic trends with poor adherence history.
- Analyze Cues: Uncontrolled hypertension is increasing risk for cardiovascular and renal complications.
- Prioritize Hypotheses: Highest priority is risk of end-organ injury from sustained pressure elevation.
- Generate Solutions: Strengthen home-monitoring routine, medication adherence plan, and lifestyle interventions.
- Take Action: Re-teach blood pressure technique, reinforce medication schedule, and coordinate follow-up review.
- Evaluate Outcomes: Home logs trend downward toward target range and adherence improves.
Related Concepts
- coronary-artery-disease - Hypertension accelerates vascular injury linked to ischemic cardiac disease.
- heart-failure - Chronic pressure overload increases risk for ventricular dysfunction.
- kidney-disease - Sustained hypertension contributes to progressive renal damage.
- stroke - Elevated pressure is a major modifiable cerebrovascular risk factor.
- peripheral-vascular-system-and-insufficiency-patterns - Vascular dysfunction patterns overlap with long-term hypertension complications.
Self-Check
- Which blood pressure ranges define Stage 1 and Stage 2 hypertension?
- Why can hypertension remain high risk even when the client reports no symptoms?
- Which teaching points best improve long-term blood pressure control and complication prevention?