Bell Palsy
Key Points
- Bell palsy is sudden peripheral facial-nerve (CN VII) dysfunction causing unilateral facial weakness or paralysis.
- Onset is typically rapid, often progressing over about 48 to 72 hours.
- Most cases are self-limited with substantial recovery within weeks to months, but residual weakness can persist.
- Priority care includes early symptom recognition, exclusion of structural/vascular mimics, and eye-protection measures.
- Early steroid therapy (within about 72 hours), supportive care, and rehabilitation-focused exercises improve recovery potential.
Pathophysiology
Bell palsy is thought to involve inflammation and swelling of the facial nerve, commonly linked to viral triggers such as herpes simplex. Neural edema impairs facial-muscle motor signaling and can also alter taste, lacrimation, and sound sensitivity.
Because unilateral facial weakness can mimic central neurologic emergencies, diagnostic evaluation must first exclude alternate causes such as stroke or brain tumor.
Classification
- Typical unilateral Bell palsy: One-sided facial weakness/paralysis with peripheral CN VII pattern.
- Bilateral involvement (rare): Bilateral facial weakness presentations requiring broader differential workup.
- Recovery trajectory domain: Self-limited near-complete recovery versus persistent residual weakness.
Nursing Assessment
NCLEX Focus
Prioritize rapid facial-neurologic assessment, eye-protection risk, and emergency mimic exclusion.
- Assess onset timing and progression speed of facial weakness, including drooping mouth/eyelid and drooling.
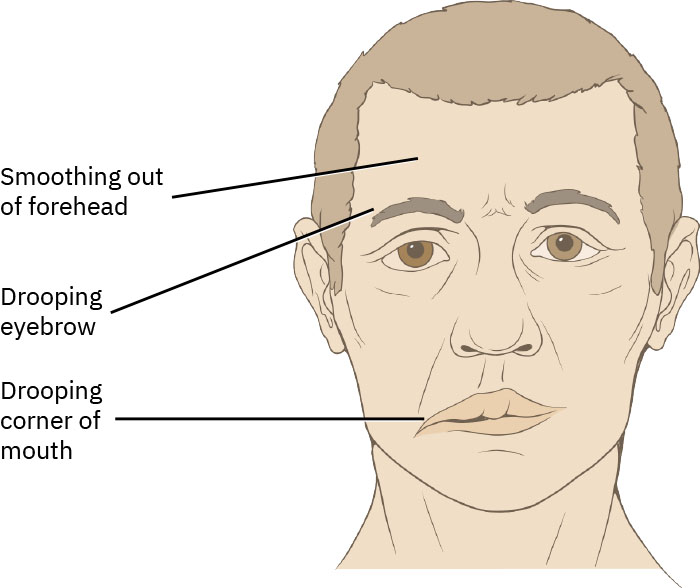 Illustration reference: OpenStax Clinical Nursing Skills Ch.22.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.22.1.
- Assess eyelid closure ability and corneal-exposure risk from dry eye or excessive tearing.
- Screen associated symptoms: altered taste (anterior tongue), hyperacusis, facial/jaw/retroauricular pain, and speech-articulation changes.
- Assess risk context including pregnancy/preeclampsia, obesity, hypertension, diabetes, stress, sleep deprivation, autoimmune patterns, and recent viral illness.
- In stroke differential screening, check for central red flags (arm drift, pupil asymmetry, altered consciousness, broader focal deficits); isolated peripheral facial findings with ear pain/inability to close eyelid support Bell palsy pattern.
- Support diagnostic workup used to characterize severity and rule out alternate causes (for example EMG, MRI/CT, targeted blood testing).
Nursing Interventions
- Escalate immediately when findings are inconsistent with isolated peripheral facial-nerve palsy or when central neurologic deficits are present.
- Support early steroid-treatment initiation when ordered within symptom-onset window.
- Implement corneal-protection plan: artificial tears, eye patching, and nighttime eye-closure protection when indicated.
- Support pain and comfort management, facial-muscle exercise guidance, and rehabilitation referrals.
- Reinforce expected recovery timeline, warning signs, and follow-up adherence for delayed or incomplete recovery.
Eye Injury Risk
Inability to close the affected eye increases corneal injury risk and requires immediate protective interventions.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Corticosteroids | Protocol-specific | Best benefit is early initiation after symptom onset to reduce nerve inflammation. |
| Antiviral therapy | Protocol-specific | May be added in selected cases based on presumed viral trigger and severity context. |
| Nonopioid analgesics | aspirin, acetaminophen, ibuprofen | Support pain control and comfort while monitoring contraindications and total daily dosing. |
Clinical Judgment Application
Clinical Scenario
A patient develops sudden right-sided facial droop over 24 hours with inability to close the right eyelid and altered taste, without limb weakness or speech aphasia.
- Recognize Cues: Rapid unilateral peripheral facial pattern with eye-exposure risk.
- Analyze Cues: Bell palsy is likely, but central causes must remain excluded.
- Prioritize Hypotheses: Immediate priorities are neurologic safety screening and corneal protection.
- Generate Solutions: Coordinate diagnostic exclusion of stroke/tumor and start supportive treatment pathway.
- Take Action: Implement eye-protection plan, support medication orders, and provide recovery education.
- Evaluate Outcomes: Facial function improves over follow-up interval without ocular complications.
Related Concepts
- head-and-neck-assessment-and-common-abnormalities - Focused facial-symmetry and cranial-nerve screening framework.
- stroke - Critical differential diagnosis for sudden facial asymmetry.
- neurological-physical-assessment-and-red-flag-screening - Structured neurologic triage and escalation cues.
- thyroid-disorders - Endocrine comorbidity context that can coexist with fatigue and facial symptom complaints.
Self-Check
- Which bedside findings support peripheral facial-nerve palsy pattern rather than generalized neurologic decline?
- Why is eye protection an immediate nursing priority in Bell palsy?
- Which patient factors and symptom patterns should prompt urgent expansion of the differential diagnosis?