ACE Inhibitors
Key Points
- ACE inhibitors block the conversion of angiotensin I → angiotensin II, reducing vasoconstriction, aldosterone release, and blood pressure.
- Used for hypertension, heart failure, post-MI cardioprotection, and diabetic nephropathy.
- Signature adverse effect: persistent dry cough (bradykinin accumulation) — occurs in up to 15% of patients; switch to ARB if intolerable.
- ACE-inhibitor cough may persist for weeks to months and may resolve only after discontinuation in some patients.
- Hyperkalemia risk — avoid potassium supplements and potassium-sparing diuretics; monitor serum potassium closely.
- Severe hyperkalemia is an emergency; potassium above about 6.0 mEq/L can precipitate life-threatening dysrhythmia and cardiac arrest.
- Rare but serious adverse effects include neutropenia/agranulocytosis and proteinuria; escalate new infection cues or renal-change trends promptly.
- ACE inhibitors can increase risk of lithium toxicity when combined with lithium therapy.
- Absolute contraindication in pregnancy (boxed warning): causes fetal harm and death; women of childbearing age must use effective contraception.
- Some low-renin hypertension phenotypes can show weaker ACE inhibitor monotherapy response and may need combination antihypertensive therapy.
- Pediatric congenital-cardiac use may include selected valve-regurgitation lesions, left-to-right shunt defects, and heart-failure pathways to reduce afterload and remodeling stress.
Mechanism of Action
The renin-angiotensin-aldosterone system (RAAS) regulates blood pressure and fluid balance:
- Renin (from kidneys) converts angiotensinogen → Angiotensin I
- ACE (angiotensin-converting enzyme) converts Angiotensin I → Angiotensin II
- Angiotensin II causes vasoconstriction + aldosterone release → sodium/water retention → elevated BP
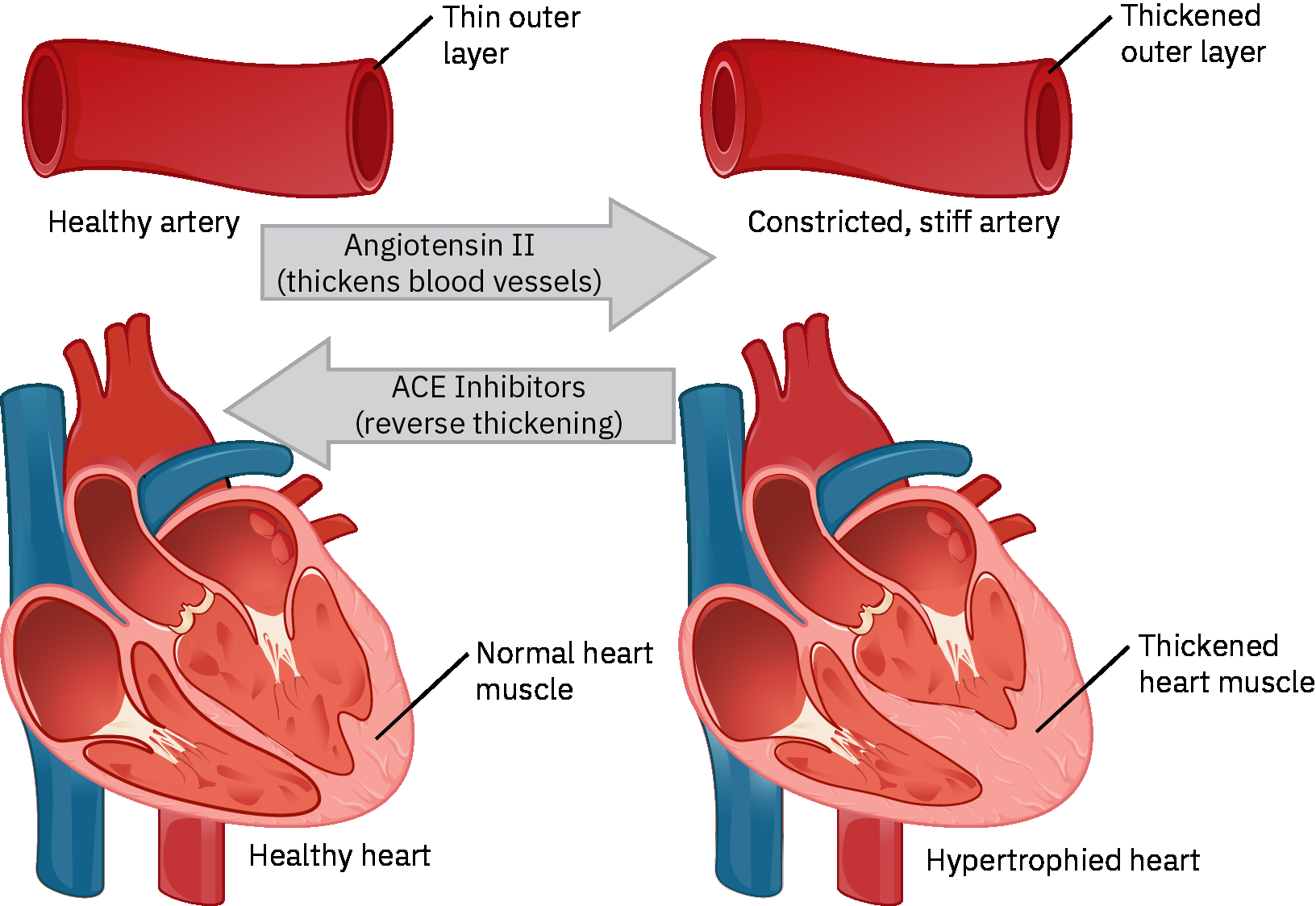 Illustration reference: OpenStax Pharmacology Ch.18.2.
Illustration reference: OpenStax Pharmacology Ch.18.2.
ACE inhibitors block step 2, preventing angiotensin II formation:
- Vasodilation → ↓ systemic vascular resistance → ↓ blood pressure
- ↓ Aldosterone → ↑ sodium and water excretion → ↓ preload and fluid volume
Bradykinin (normally degraded by ACE) accumulates → causes the characteristic dry cough.
Common ACE Inhibitors
| Drug | Route | Typical Dose |
|---|---|---|
| Lisinopril (Zestril) | PO | 10–40 mg once daily |
| Enalapril (Vasotec) | PO, IV | 5–40 mg/day in 1–2 doses |
| Captopril (Capoten) | PO | 6.25–12.5 mg every 8 hours as common starting range; titrate by indication |
| Benazepril (Lotensin) | PO | 10–40 mg once daily |
| Ramipril (Altace) | PO | 2.5–20 mg/day in 1–2 doses |
Indications
- Hypertension — first-line therapy (especially in patients with diabetes or CKD)
- Heart failure (reduced ejection fraction) — reduces mortality and hospitalizations
- Post-myocardial infarction — cardioprotection and remodeling prevention
- Post-MI reduced EF pathways — often initiated when left-ventricular ejection fraction is below about 40% to reduce remodeling and heart-failure progression risk
- Diabetic nephropathy — slows progression of kidney damage by reducing intraglomerular pressure
- Selected pediatric congenital-heart pathways — afterload reduction in mitral/aortic regurgitation and left-to-right shunt burden when specialist-directed
Nursing Assessment
NCLEX Focus
Two signature ACE inhibitor adverse effects to know:
- Dry, persistent cough (bradykinin effect) — does NOT resolve with dose reduction; switch to ARB (angiotensin receptor blocker) if intolerable
- Angioedema — rare but life-threatening swelling of face, lips, tongue, or throat — discontinue immediately and treat as emergency
Pre-administration:
- Assess blood pressure and pulse — hold and notify provider if significantly hypotensive
- Review potassium level — ACE inhibitors cause potassium retention (hyperkalemia risk)
- Assess pregnancy status — absolutely contraindicated in pregnancy (boxed warning)
- Assess renal function — use with caution in renal impairment; may worsen renal function
- Identify potential lower-renin monotherapy nonresponse and prepare for combination-therapy planning when blood-pressure reduction is inadequate.
Contraindications:
- Pregnancy (boxed warning — fetal harm/death)
- History of ACE inhibitor-associated angioedema or hereditary angioedema
- Concurrent use with aliskiren in diabetic patients (severe hypotension/renal impairment risk)
- Bilateral renal artery stenosis
Nursing Interventions
Monitoring parameters:
- Blood pressure (especially first dose — first-dose hypotension risk, especially in volume-depleted patients)
- Serum potassium — hyperkalemia risk; avoid potassium supplements, salt substitutes, and potassium-sparing diuretics
- Renal function (BUN/creatinine) — mild elevation expected; significant rise requires provider notification
- If co-prescribed with lithium, monitor for lithium toxicity (tremor, confusion, GI upset) and coordinate level checks
- Signs of angioedema: sudden facial or airway swelling — emergency; discontinue and call rapid response
- Monitor CBC/clinical infection cues when prolonged therapy or high-risk context raises concern for neutropenia/agranulocytosis.
Interaction-focused safety checks:
- Avoid concomitant sacubitril/valsartan pathways unless prescriber-directed transition safeguards are in place.
- Reconcile interacting medications: aliskiren, NSAIDs (including COX-2 inhibitors), potassium-sparing diuretics, lithium, and mTOR-pathway agents (temsirolimus, sirolimus, everolimus).
Adverse effects to monitor:
- Dry persistent cough — most common; report to provider; may require medication change to ARB
- Hypotension — especially first dose and in dehydrated patients; check BP before each dose
- Hyperkalemia — fatigue, muscle weakness, cardiac dysrhythmias
- Angioedema — rare but life-threatening (swelling of face, lips, throat)
- Altered taste sensation — typically resolves within 2–3 months
Angioedema Emergency
Any report of sudden swelling of the face, lips, tongue, or throat in a patient taking an ACE inhibitor requires immediate discontinuation of the medication and emergency treatment. Airway compromise can occur rapidly.
Patient education:
- Take medication at the same time each day; do not stop abruptly
- Report persistent dry cough to provider — alternative medication may be needed
- Avoid potassium supplements and salt substitutes (most contain potassium chloride)
- If also taking lithium, report new tremor, confusion, or GI symptoms promptly
- Avoid nonprescribed NSAID overuse because blood-pressure control and kidney safety can worsen with ACE inhibitor combinations
- Rise slowly from sitting or lying position — orthostatic hypotension risk
- Women of childbearing age: use effective contraception; report pregnancy immediately — medication must be stopped immediately
- Report any facial swelling, difficulty breathing, or swallowing immediately
Related Concepts
- hypertension-assessment-and-management — ACE inhibitors as first-line antihypertensive therapy, especially in diabetes and CKD.
- heart-failure — ACE inhibitors reduce mortality and prevent cardiac remodeling in systolic heart failure.
- kidney-disease — Renoprotective effects in diabetic nephropathy; monitoring for worsening renal function.
- potassium-balance-disorders — Hyperkalemia risk from ACE inhibitor-induced aldosterone suppression.
- antihypertensives — ACE inhibitors in context of antihypertensive drug classes.
- high-alert-medications — ACE inhibitor-associated risks (angioedema, hypotension, teratogenicity) requiring monitoring.
Self-Check
- A client taking lisinopril reports a persistent dry cough for 3 weeks. What is the most likely cause, and what nursing action is appropriate?
- A client on captopril has a serum potassium of 5.8 mEq/L. What factors may have contributed to this, and what nursing interventions are indicated?
- Why are ACE inhibitors absolutely contraindicated in pregnancy, and what teaching should the nurse provide to a woman of childbearing age starting lisinopril?