Pressure Injury Staging and Risk Assessment
Key Points
- Pressure injuries result from ischemic tissue damage caused by pressure, friction, and shear.
- Risk rises with moisture exposure, impaired mobility, reduced cognition, and poor nutrition or hydration.
- The Braden Scale standardizes risk stratification; lower scores indicate higher injury risk.
- Accurate staging (I-IV, deep tissue, unstageable) guides intervention urgency and monitoring.
- Severe sustained compression can produce clinically relevant tissue injury rapidly, sometimes within about 1 hour.
- Pressure injuries are treated as preventable safety events, so early prevention and precise staging documentation are critical.
- Critical-care populations have high pressure-injury burden, with reported ICU development rates commonly around 8%-23% in hospitalized cohorts.
- Smart-bed support surfaces (for example pressure redistribution and microclimate control) can reduce sustained tissue load and moisture-related breakdown risk.
Pathophysiology
Pressure injury develops when sustained force compresses soft tissue between external surfaces and bony prominences, reducing blood and lymph flow. Ischemia leads to inflammation, edema, necrosis, and possible ulceration.
Pressure injuries commonly develop at the sacrum, heels, ischia, and coccyx where bony prominence pressure is highest.
Friction and shear worsen injury by damaging superficial skin and deeper vascular structures. A common shear mechanism is sliding down in bed, where skin remains fixed against linens while deeper tissue moves with bone, stretching and tearing capillary beds. Shear can also bend or occlude vessels enough to create local thrombosis and impaired tissue circulation.
Current staging language uses the term pressure injury rather than pressure ulcer because tissue damage can exist before an open ulcer is visible.
Classification
- Stage I: Intact skin with localized nonblanchable erythema over prolonged-pressure area.
- Stage II: Partial-thickness skin loss with exposed dermis; shallow open wound or intact/ruptured blister pattern with viable red/pink moist bed and no visible slough/eschar or deeper tissue structures.
- Stage-II exclusion rule: Do not use stage II to label moisture-associated skin damage patterns (for example IAD/ITD/MARSI) or traumatic skin injuries (for example skin tears, burns, abrasions).
- Stage III: Full-thickness tissue loss with visible adipose; no exposed cartilage, tendon, ligament, muscle, or bone.
- Stage IV: Full-thickness loss with extensive tissue destruction and exposed or palpable fascia, tendon, ligament, muscle, cartilage, or bone; slough/eschar and undermining/tunneling may be present with highest infection and osteomyelitis risk.
- Unstageable: Full-thickness loss with true depth obscured by slough or eschar; stage may become III/IV after appropriate debridement.
- Deep tissue pressure injury: Persistent nonblanchable deep red/maroon/purple discoloration (intact or nonintact skin) or blood-filled blister from intense/prolonged pressure and shear; pain/temperature changes may precede visible discoloration.
- Mucosal membrane pressure injury: Device-associated injury on mucous membranes; these injuries are not staged because mucosal anatomy differs from skin staging assumptions.
- Medical device-related pressure injury (MDRPI): Pattern typically conforms to the device footprint and should be staged using the standard system.
- Stage modifiers: Undermining and tunneling may occur in deeper injuries; epibole (rolled wound edges) can impede closure; slough/eschar burden can obscure true depth.
- Kennedy terminal ulcer pattern: Rapidly progressive sacral terminal pressure injury near death, often pear/butterfly/horseshoe shaped with irregular borders and dark-red/yellow/black/purple color progression.
Nursing Assessment
NCLEX Focus
Prioritize risk recognition and stage accuracy, then match prevention or escalation intensity to findings.
- Assess moisture exposure, mobility, sensory perception, nutrition, cognition, and friction/shear.
- Assess contributors such as weakness, stroke-related sensory loss, frequent incontinence, and reduced intake that accelerate pressure-injury risk.
- In ICU pathways, include fluid-overload edema and poor nutrition as additional high-risk tissue-breakdown contributors.
- Include high-risk contributors during screening: advanced age, poor hygiene, fractures/immobility trauma, diabetes, immunosuppression, corticosteroid exposure, organ dysfunction, prior pressure-injury history, fever, extremes of body weight, terminal illness/end-of-life trajectory, and microvascular dysfunction.
- Recognize elevated risk in operating-room and critical-care populations where hemodynamic instability, vasoactive therapy, and multiple medical devices increase pressure and perfusion burden.
- Use the Pressure Injury Staging And Risk Assessment on admission and at scheduled reassessment points.
- Document present-on-admission skin injury and stage baseline findings clearly to distinguish preexisting injury from hospital-acquired progression.
- Evaluate blanching response and persistent nonblanchable changes over bony prominences.
- When staging is uncertain, document objective wound characteristics first and escalate for staging confirmation rather than assigning a speculative stage.
- Distinguish expected transient hyperemia from persistent injury cues; after prolonged pressure exposure (for example >=2 hours), warmth/redness that does not resolve over roughly 60-90 minutes after repositioning should prompt escalation.
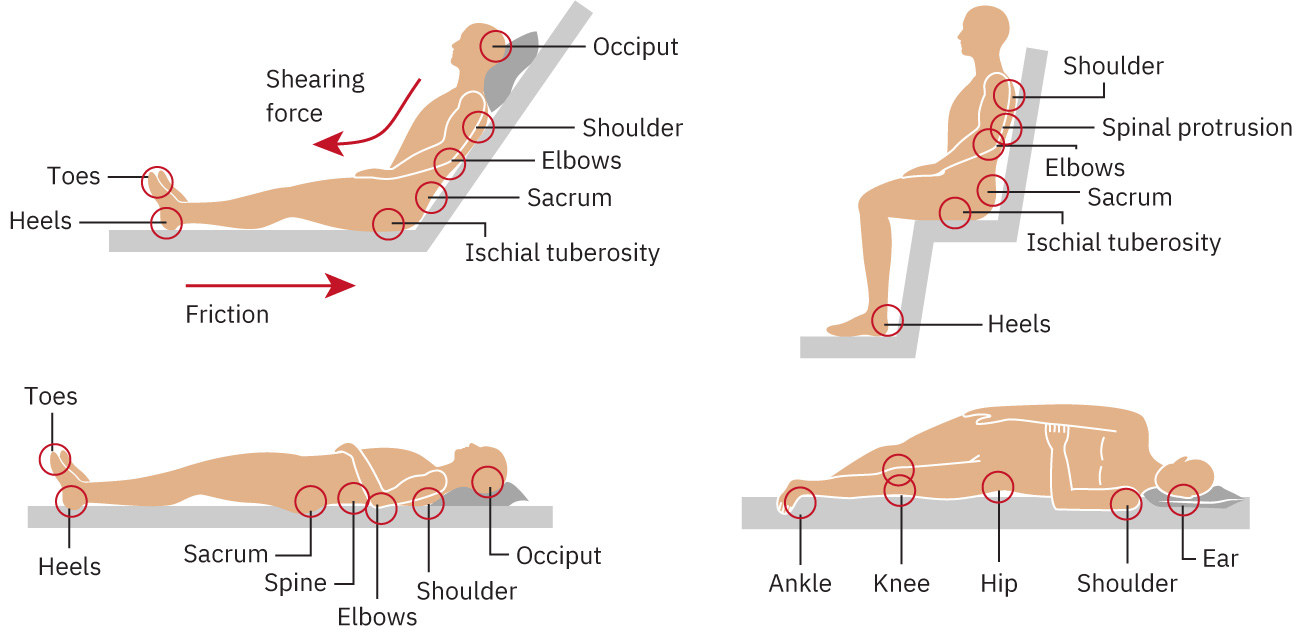 Illustration reference: OpenStax Medical-Surgical Nursing Ch.28.3.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.28.3.
- In darkly pigmented skin, add cue-based screening for stage-1 risk:
- pain or tenderness compared with nearby skin
- firmness or softness change
- local temperature change
- color shift relative to surrounding tissue
- In stage-2 injury, assess for shallow open dermal loss or intact/ruptured blister pattern with possible pain, swelling, or discoloration.
- In stage-3/4 injury, assess for purulent drainage, necrosis, fever/infection cues, undermining, and tunneling.
- Assess slough/eschar characteristics because depth may be obscured until nonviable tissue is removed.
- In suspected deep-tissue injury, monitor for rapid evolution of depth while recognizing some areas may resolve without tissue loss.
- Do not relabel traumatic, neuropathic, dermatologic, or vascular lesions as deep-tissue pressure injury without pressure/shear evidence.
- Include nutrition markers (for example low albumin) when delayed wound healing risk is suspected.
- Evaluate nutrition/perfusion barriers such as hypoproteinemia, negative nitrogen balance, dehydration, edema, and vitamin C deficiency when stage progression or delayed healing is present.
- Trend stage, wound-bed characteristics, and surrounding tissue changes to detect progression.
Nursing Interventions
- Implement individualized prevention bundles based on Braden risk level.
- Reposition regularly, offload pressure points, and reduce friction/shear during transfers.
- For immobilized clients, use scheduled turning (commonly at least every 2 hours) and reassess tolerance/skin response.
- If a critically ill patient is not hemodynamically stable enough to tolerate full turns, escalate promptly and use alternative offloading/protection strategies per protocol.
- Use draw-sheet assisted repositioning (often with two-person assist) to reduce shear and friction.
- Keep head-of-bed elevation at about 30 degrees or less when clinically feasible to reduce sacral shear.
- Keep linens clean, dry, and wrinkle-free to reduce friction and moisture-related injury.
- Keep skin clean and dry; use barrier protection for incontinence-associated moisture.
- Apply prophylactic dressings to selected high-risk pressure areas when ordered/policy-supported.
- After incontinence or secretion exposure, cleanse promptly and use absorbent pads/barrier products to limit maceration and excoriation risk.
- Use pressure-offloading devices that maintain shape under body weight (for example foam wedges, gel interfaces, pressure-reducing boots) and avoid ring/donut cushions that can worsen venous congestion around tissue.
- Use available smart-bed surface features (for example pressure-redistribution modes and microclimate controls) to supplement turning/offloading plans.
- Escalate stage progression, unstable tissue findings, or signs of infection promptly.
- Coordinate debridement pathway when slough/eschar prevents accurate staging or healing progression; follow orders for chemical/mechanical methods within nursing scope.
- Avoid routine removal of dry, adherent heel eschar on ischemic limbs unless provider-directed because it may be biologically protective.
- Treat stable eschar as adherent, dry, intact tissue without fluctuance or erythema; monitor closely rather than softening/removing by routine.
- Escalate suspected stage-4 bone involvement for urgent evaluation and antimicrobial management planning.
- Treat hospital-acquired or worsening pressure injuries as preventable safety events requiring immediate review and quality-reporting follow-through per facility policy.
Staging Safety Issue
Inaccurate staging delays treatment; missed prevention can progress to serious reportable harm events.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| topical-skin-protectants | Barrier creams | Reduce moisture-associated skin breakdown risk. |
| analgesics | Acetaminophen, opioids | Support tolerability of repositioning and wound care. |
Clinical Judgment Application
Clinical Scenario
A bedbound patient with urinary incontinence has new sacral nonblanchable erythema and a Braden score of 14.
- Recognize Cues: Moisture burden, mobility limits, and low risk score.
- Analyze Cues: Pattern is consistent with high risk and early pressure injury development.
- Prioritize Hypotheses: Immediate priority is preventing progression from early-stage tissue injury.
- Generate Solutions: Intensify offloading, moisture control, and reassessment frequency.
- Take Action: Start targeted prevention bundle and document stage-specific findings.
- Evaluate Outcomes: Skin changes stabilize without deeper-stage progression.
Related Concepts
- braden-scale-risk-domains-and-score-guided-interventions - Domain-based risk scoring and prevention-intensity mapping.
- integumentary-system - Baseline barrier vulnerability and skin-care priorities.
- moving-and-positioning-clients - Positioning technique directly affects pressure and shear loads.
- immobility-complications - Immobility amplifies pressure injury risk and consequences.
- wound-classification-framework - Pressure injury is a distinct wound class with staging requirements.
- delayed-wound-healing-factors-and-complications - Stage progression increases risk of delayed healing.
Self-Check
- Why does a lower Braden score change prevention intensity?
- How does nonblanchable erythema differ from transient pressure hyperemia?
- Which risk factors should trigger more frequent skin reassessment?