Comprehensive Abdominal Assessment
Key Points
- Abdominal assessment combines focused GI and GU interview data with a sequenced physical exam.
- Interview findings guide exam priorities, especially for pain, elimination changes, and urinary symptoms.
- PQRST improves abdominal pain characterization and helps connect location with likely pathology.
- Abdominal exam order preserves bowel sound accuracy by performing auscultation before palpation.
Pathophysiology
Abdominal symptoms often reflect dysfunction in gastrointestinal and genitourinary structures that share anatomic space and overlapping symptom patterns. Because many disorders present with nonspecific findings, nurses must integrate history and exam trends to detect deterioration early.
The abdominal assessment model is built to reduce missed cues. Subjective findings identify likely targets, while objective findings confirm or challenge initial hypotheses. This cyclical process supports rapid reprioritization when new data emerge.
The abdomen is anatomically defined as the anterior trunk region between the diaphragm and pelvis. Abdominal findings can reflect gastrointestinal and genitourinary function and may also provide clues about reproductive, metabolic, and immune system status.
Intra-abdominal pressure (IAP) is a dynamic pressure state created by interaction of abdominal wall and viscera. Volume-raising conditions (for example obstruction, ascites/fluid accumulation, organ inflammation, mass effect, or pregnancy) can exceed compensatory stretch capacity and contribute to organ dysfunction.
Risk context should be screened early because modifiable and nonmodifiable factors alter GI symptom burden and complication probability. Diet pattern, inactivity, medication effects (for example iron and opioids), family history, aging physiology, and severe stress exposure can shift baseline risk before acute findings appear.
Classification
- Subjective domain: Prior diagnoses, surgeries, medications, pain pattern, bowel and urinary symptom review.
- Objective domain: Inspection, auscultation, percussion, and palpation with quadrant-based interpretation.
- External-structure domain: Skin, superficial/transversalis fascia, abdominal wall muscles, fat, and peritoneum layers that support protection, movement, thermoregulation, and organ anchoring.
- Anatomic-reference domain: Four abdominal quadrants formed by intersecting horizontal/vertical reference lines at the umbilicus for symptom localization.
- Quadrant-organ correlation domain:
- RUQ: Liver, gallbladder, right kidney (posterior), and portions of small/large bowel.
- LUQ: Stomach, spleen, pancreas, left kidney (posterior), portions of bowel, and part of liver.
- RLQ: Appendix, cecal/ascending colon segments, right adnexa (if present), and upper right bladder region.
- LLQ: Descending/sigmoid colon segments, left adnexa (if present), and upper left bladder region.
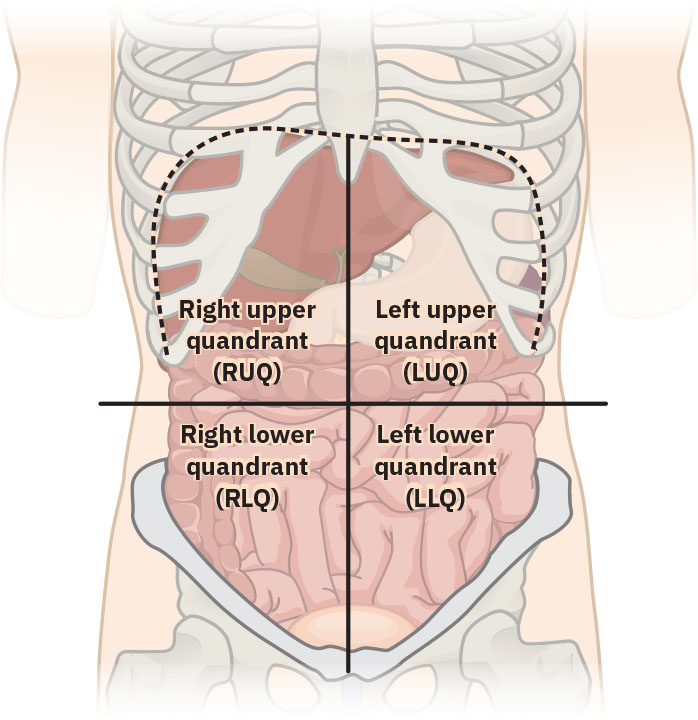 Illustration reference: OpenStax Clinical Nursing Skills Ch.27.2.
Illustration reference: OpenStax Clinical Nursing Skills Ch.27.2.
- Abdominal-wall support domain: Rectus abdominis supports posture and anterior-organ containment; external/internal obliques support trunk rotation; transversus abdominis supports trunk stability and intra-abdominal pressure regulation.
- Major abdominal-vascular landmarks: Abdominal aorta (primary arterial outflow to lower systemic circulation) and inferior vena cava (major venous return from lower body) are key interpretation targets for pulsation, bruit, and instability cues.
- Viscera-type domain: Solid viscera (for example liver, spleen, kidneys, pancreas, gallbladder) versus hollow viscera (for example stomach, intestines, bladder); hollow-viscera injury has leak-peritonitis risk.
- Arterial-supply domain: Major abdominal perfusion branches include celiac and mesenteric arterial pathways serving hepatobiliary, gastric, pancreatic, and intestinal structures.
- Venous-drainage domain: Portal/mesenteric/hepatic/renal/gonadal venous return pathways integrate into systemic venous flow via IVC tributary architecture.
- Functional-abdominal domain: Supports forced expiration/cough, bladder emptying, emesis, defecation/flatulence, and pregnancy-related abdominal wall adaptation.
- Common-impairment contributor domain: Medication effects (for example opioid-constipation, antibiotic-associated diarrhea, NSAID/antacid overuse dyspepsia-reflux), poor diet/inactivity, reflux burden, and stress-related GI symptom amplification.
- Symptom-pattern domain: Colicky/wavelike, cramp-like, generalized, and localized abdominal pain descriptors plus associated symptoms (bloating, nausea, anorexia, bowel-habit change, distention).
- Pain framework: PQRST (provocation, quality, region/radiation, severity, timing).
- Diagnostic-support domain: Targeted labs (CBC, CMP, albumin, thyroid function, stool studies, lipase, CRP/ESR), breath testing, genetics pathways, and imaging/endoscopy selected from exam cues.
Nursing Assessment
NCLEX Focus
Prioritization often depends on recognizing red-flag abdominal cues and using systematic follow-up questions.
- Ask targeted GI and GU history questions, including prior abdominal surgery, bowel pattern changes, dysphagia, dysuria, urgency, and incontinence.
- For dysuria, clarify internal versus external discomfort pattern and prior self-treatment attempts.
- For urinary symptoms, characterize daytime-versus-nocturnal frequency, urgency with leakage, stress incontinence triggers (cough/sneeze/exertion), and hesitancy at stream initiation.
- Characterize stool patterns with a consistent descriptor framework (for example, Bristol stool forms) when evaluating constipation or diarrhea trends.
- Screen cultural influences on symptom expression and dietary practices, including preferred terminology, family support structure, and complementary-treatment use.
- Screen socioeconomic barriers that affect GI outcomes, such as food insecurity, medication affordability, access to screening procedures, and oral-health access for chewing/intake.
- Ask focused bleeding and elimination safety questions, including hematochezia, melena, hematemesis, abdominal distention, recent bowel movement timing, and flatus passage.
- Ask associated symptom questions for bloating/fullness, nausea/vomiting, appetite loss (anorexia), and stool-habit change to refine differential direction.
- For diarrhea-focused history, document watery versus formed stool pattern and 24-hour episode count to guide dehydration/infectious-workup priorities.
- Clarify stool quality details during interview: color, consistency, caliber, odor, mucus, and undigested-food patterns to separate expected variation from alarm findings.
- Treat black/red stool, persistent white stool, recurrent watery stool, hard pellet stool, or progressively narrow stool caliber as escalation cues in the full clinical context.
- Treat new bright red rectal bleeding or new melena as urgent provider-notification findings because both may indicate clinically significant GI bleeding.
- Escalate persistent or high-risk emesis patterns (for example vomiting beyond 24 hours, blood in emesis, severe pain, or dehydration signs) for urgent provider reassessment.
- Treat bloody stool, hematemesis, new/worsening melena, or dehydration with oliguria (for example urine output below about 30 mL/hour) as critical findings requiring immediate escalation.
- Screen swallowing safety in clients with stroke or TIA history and monitor pill/liquid/food tolerance to reduce aspiration-pneumonia risk.
- Use comprehensive-pain-assessment-and-documentation with PQRST for abdominal pain, and map findings to quadrants.
- Clarify pain descriptors explicitly (colicky, cramp-like, generalized, localized) because each pattern changes urgency and likely source interpretation.
- Use quadrant localization consistently when documenting pain, tenderness, masses, or distention to support differential narrowing and handoff clarity.
- Prepare for exam accuracy by promoting comfort (warm room/stethoscope, bladder emptying, relaxed positioning).
- Use standardized pre-exam safety sequence: hand hygiene/PPE as indicated, identity verification, exam explanation with consent, supine positioning, and modesty-preserving exposure.
- Include focused oral-oropharyngeal screening when GI concerns include intake/swallowing issues: inspect lips, buccal mucosa, gums/teeth, tongue mobility, palate/uvula, and tonsillar/oropharyngeal findings.
- Treat new lip asymmetry with facial droop, arm weakness/numbness, or speech change as a potential acute stroke pattern requiring immediate escalation.
- If epiglottitis is suspected (for example stridor, hyperthermia, drooling, severe sore throat), avoid tongue-depressor provocation due airway-spasm risk and escalate urgently.
- Inspect contour and distention with the patient supine and relaxed, documenting symmetry, contour type (flat/rounded/scaphoid/protuberant), scars, umbilicus position, masses, and visible pulsations/peristalsis.
- During inspection, confirm relaxed abdominal wall (arms at sides; head/knee support as needed) and document striae, hernia-like bulges, scar correlation, and umbilicus (typically inverted and midline).
- Use method-specific expected/unexpected framing during exam:
- Inspection expected findings: flat/rounded contour with symmetry and intact skin.
- Inspection unexpected findings: asymmetry, progressive distention, visible peristalsis/pulsation, wounds, or skin breakdown.
- Auscultation expected finding: normal bowel sounds.
- Auscultation unexpected findings: absent/hyperactive/hypoactive bowel sounds.
- Palpation expected findings: no masses, no tenderness, no involuntary guarding.
- Palpation unexpected findings: pain, rebound tenderness, rigidity, involuntary guarding, or new masses.
- GU expected findings: clear pale-yellow urine and nondistended bladder without urgency/frequency/retention.
- GU unexpected findings: dark/bloody/foul/sedimented urine, dysuria, urgency/frequency, distended tender bladder, or retention signs.
- Auscultate bowel sounds before palpation to avoid altering baseline findings; begin in RLQ and proceed clockwise.
- If bowel sounds are not initially heard, continue listening up to about 5 minutes in that quadrant before concluding marked hypoactivity/absence.
- Describe bowel sounds as normal/hyperactive/hypoactive rather than counting exact frequency because bowel activity is cyclic.
- Recognize that normal bowel activity can have long peak-to-peak variation (up to about 50 to 60 minutes), so short silent intervals should not be overcalled as absent sounds.
- Recognize auscultation red flags: hyperactive sounds or borborygmus, hypoactive sounds after surgery/ileus patterns, and unexpected vascular sounds such as bruits.
- If peristaltic-sound conduction is clear across the abdomen, single-location auscultation may be sufficient for trend checks, while complete quadrant review remains standard for initial focused assessment.
- Interpret bowel-sound changes with motility context: absent or markedly altered sounds can indicate obstruction, ileus, or inflammatory processes and help evaluate response to bowel-rest or NG-decompression plans.
- During palpation, assess pain area last and distinguish voluntary guarding from involuntary guarding, rigidity, and rebound tenderness.
- For light palpation, begin in RLQ and move clockwise with shallow pressure (about 1 cm); keep painful area for last and encourage knee flexion to reduce muscle guarding.
- Avoid deep palpation when contraindications are suspected (for example abdominal aortic aneurysm, appendicitis concern, tender spleen, polycystic-kidney rupture risk, or recent kidney transplant).
- Palpate suprapubic-to-umbilical midline for bladder distention when retention is suspected; a distended bladder may present as a smooth, firm, regular, midline pelvic mass.
- Differentiate guarding patterns: voluntary guarding (anxiety/cold-touch related), involuntary guarding (reflex contraction with peritoneal irritation), rigidity (persistent involuntary muscle hardening), and rebound tenderness (pain on abrupt release).
- Use percussion findings (tympany versus dullness) to support concern for stool burden, mass effect, or abnormal fluid patterns; a shift from expected tympany toward diffuse/shifting dullness supports ascitic-fluid concern.
- Percussion may support liver/spleen span assessment and costovertebral-angle tenderness screening in upper-level abdominal-kidney evaluation.
- Trend common GI laboratory indicators with the clinical picture, including anemia/inflammation cues on CBC, hepatobiliary markers/electrolytes on CMP, and lipase for pancreatic involvement.
- Use stool diagnostics (occult blood, culture including C. diff testing, ova/parasite testing) and inflammatory markers (CRP/ESR) to refine differential priorities.
- Add albumin and thyroid-function trends when malnutrition, malabsorption, or bowel-motility concerns are part of the working differential.
- Match imaging modality to the clinical question and prep needs: abdominal X-ray (obstruction/perforation screening), CT (detail with contrast and renal/allergy review), MRI/MRCP (no radiation; metal/implant and claustrophobia screening), ultrasound (radiation-free hepatobiliary/pancreatic assessment), and barium studies (bowel-prep/NPO and posttest fluid-fiber elimination support).
- For abdominal CT with contrast, verify NPO status (often 4-6 hours per order), prior iodine/contrast reaction history, renal labs (BUN/creatinine/eGFR), and medication constraints such as metformin timing restrictions.
- For prior contrast-reaction history, verify whether premedication pathways (for example antihistamine/corticosteroid protocols) are ordered and completed before contrast exposure.
- Confirm removal of metal/jewelry items before imaging modalities where this is required by protocol.
- Teach expected contrast sensations (brief warmth or metallic taste with IV contrast; chalky taste with oral contrast) and support posttest hydration to aid contrast elimination.
- After barium studies, anticipate temporary light/white stool and reinforce ordered laxative plus hydration plan to reduce postprocedure impaction risk.
- For suspected lactose malabsorption or small-intestinal bacterial overgrowth, anticipate ordered hydrogen/methane (including lactulose-based) breath-testing workflows and prep teaching.
- In patients with strong hereditary colorectal-cancer/polyposis patterns, coordinate genetics-risk referral pathways and document family-history clues that affect surveillance planning.
- Integrate endoscopy planning and surveillance: colonoscopy/EGD/ERCP sedation workflows with consent and NPO checks, plus postprocedure monitoring for bleeding, perforation, pancreatitis/cholangitis risk after ERCP, and capsule-retention risk in suspected stricture/obstruction/fistula patterns.
- Correlate quadrant pain patterns with likely causes, then anticipate diagnostics when clinically indicated.
- In older-adult constipation-focused assessment, screen for abdominal/pelvic-floor weakness, immobility, malnutrition, chronic disease burden, and long-term medication contributors.
- Ask constipation-complication questions directly (hemorrhoid bleeding, fissure pain, fecal impaction history, rectal ulcer risk).
- Apply life-span interpretation during GI assessment: infant/young-child protuberant contour can be expected, diaper counts support hydration tracking, and older adults require closer screening for constipation, xerostomia/taste change, reflux risk, ulcer risk, and bacterial-overgrowth-related diarrhea or weight loss.
- In infants and toddlers, include wet-diaper count trends, confirm umbilical-cord stump drying/fall-off timing (about two weeks), and recognize abdominal respiratory movement as an expected observation pattern.
- In pediatric abdominal complaints, expect nonspecific symptom language (for example “my stomach hurts”) and include caregiver-reported functional cues such as reduced school attendance.
Nursing Interventions
- Perform a standardized interview and exam sequence for every focused abdominal concern.
- Document findings by quadrant and by exam method to improve handoff clarity.
- Escalate findings such as severe focal tenderness, bleeding signs, persistent vomiting, or progressive distention.
- Validate that subjective and objective data are concordant before finalizing interpretation; if discordant, repeat focused exam elements and clarify interview responses.
- Prepare patients for ordered diagnostics and specimen collection with privacy-preserving communication.
- Reassess after interventions and update the care plan as cues evolve.
- During pregnancy/postpartum assessment, recognize expected abdominal-wall stretching and transient linea-alba/rectus separation patterns while escalating persistent pain, functional decline, or concerning associated findings.
- For older adults, reinforce activity-plus-fiber lifestyle strategies and monitor age-related abdominal changes (slower motility/metabolism, weaker muscle tone/ligament support, increasing visceral-fat burden) that raise constipation, hernia, and prolapse risk.
- When stool testing is ordered, provide privacy-preserving, stigma-reducing instructions for specimen collection and transport to improve adherence and sample quality.
Sequence Error Risk
Palpating before auscultation can distort bowel sound interpretation and reduce diagnostic value of the exam.
Pharmacology
Pharmacologic management depends on the identified cause and is not primary in this assessment-focused section. Medication decisions should follow confirmed clinical findings and provider orders.
Clinical Judgment Application
Clinical Scenario
A patient reports new right lower abdominal pain with nausea and reduced appetite. Interview cues and focused exam findings are used to decide next actions.
- Recognize Cues: Localized pain pattern, associated symptoms, and bowel trend changes.
- Analyze Cues: Pattern suggests potential acute abdominal pathology rather than nonspecific discomfort.
- Prioritize Hypotheses: Immediate priority is ruling out time-sensitive causes and preventing progression.
- Generate Solutions: Complete focused exam sequence, document quadrant findings, and escalate concerning cues.
- Take Action: Notify the provider promptly and support ordered diagnostics.
- Evaluate Outcomes: Reassess pain trajectory and physiologic stability after interventions.
Related Concepts
- digestive-system - Provides foundational GI anatomy and elimination context.
- abdominal-distention-and-the-five-fs - Expands differential cues for generalized abdominal swelling.
- abdominal-hernias - Covers localized bulge patterns and structural wall defects.
- diarrhea-assessment-and-management - Common symptom requiring stool-pattern and hydration assessment.
- constipation - Frequent elimination issue linked to distention and discomfort.
- social-determinants-of-health - Frames food access, coverage, and screening barriers that modify GI risk and follow-up.
- culturally-responsive-assessment-data-collection - Supports culturally safe interview technique and interpretation of symptom language.
- dysphagia - Swallowing complaints and stroke history require early aspiration-risk screening in GI interviews.
Self-Check
- Why is abdominal exam sequencing different from many other physical exams?
- How does PQRST improve differential reasoning for abdominal pain?
- Which interview findings should trigger immediate escalation during abdominal assessment?