Emergency Situations and Rapid Response
Key Points
- CNA emergency response begins with rapid recognition, immediate nurse notification, and resident protection from further harm.
- Time-sensitive emergencies include myocardial infarction, stroke, seizure, falls, fire, and airway obstruction.
- Use standard memory tools: FAST for stroke and RACE/PASS for fire response.
Pathophysiology
Emergency deterioration often reflects abrupt oxygen-delivery or neurologic compromise, trauma risk, or airway failure. In myocardial infarction and stroke, tissue death progresses quickly when perfusion is interrupted.
Seizures involve sudden abnormal neuronal firing that can impair awareness and motor control. Choking causes acute ventilation failure and may rapidly progress to hypoxia and cardiac arrest.
Because irreversible injury increases with delay, CNA actions focus on immediate escalation, hazard control, and precise event reporting.
Classification
- Cardiovascular emergency: coronary-artery-disease warning signs with chest pain, SOB, diaphoresis, or atypical symptoms.
- Neurologic emergency: stroke signs using FAST and unilateral deficits.
- Seizure emergency: Protect from injury, time event, avoid objects in mouth, report awareness and movements.
- Safety/environment emergency: Falls, fire response (RACE/PASS), and choking airway-clearance actions.
Nursing Assessment
NCLEX Focus
Priority questions ask for first action: notify nurse/activate emergency response while protecting airway and safety.
- Recognize MI cues: substernal pressure, arm/jaw radiation, SOB, diaphoresis, anxiety, nausea, fainting.
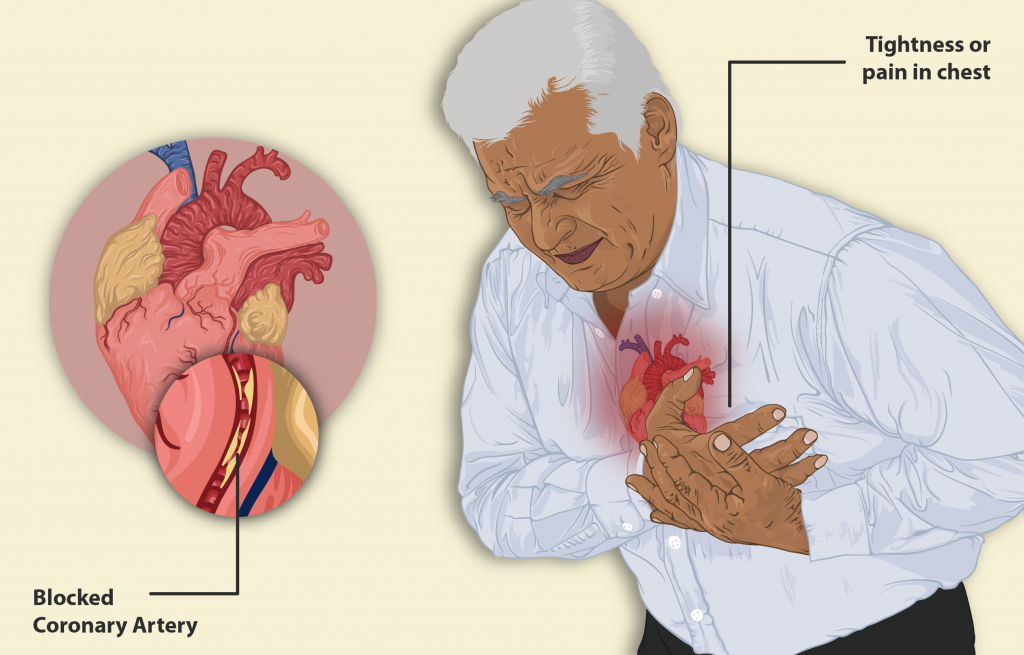 Illustration reference: OpenRN Nursing Assistant Ch.3.2.
Illustration reference: OpenRN Nursing Assistant Ch.3.2. - Recognize stroke cues with FAST: facial droop, unilateral arm weakness, slurred speech, time-critical onset.
- During seizure, assess start time, level of awareness, and specific motor/nonmotor behavior.
- After fall, avoid moving resident unless immediate danger exists and report immediately.
Nursing Interventions
- Notify nurse immediately for suspected MI, stroke, seizure onset, choking, fire, or significant fall.
- For seizure, guide to floor if possible, protect head, clear hazards, and do not place anything in mouth.
- For stroke suspicion, emphasize time of symptom onset and rapid escalation.
- For fire events, follow RACE and use PASS only if safe and trained.
- For choking, encourage forceful coughing if effective; when ineffective, perform airway-clearance protocol per training.
Delay-to-Harm Risk
Delayed recognition or delayed notification in MI, stroke, airway obstruction, or fire can lead to irreversible injury or death.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| thrombolytics | tPA contexts for ischemic stroke | Benefit is strongly time-dependent; document onset and report urgently. |
| anxiolytics | Post-seizure prevention contexts | Monitor sedation and safety after administration and report recurrent seizure activity. |
Clinical Judgment Application
Clinical Scenario
A resident suddenly develops right-arm weakness, facial asymmetry, and slurred speech during lunch.
- Recognize Cues: FAST-positive signs with abrupt onset.
- Analyze Cues: High probability of acute stroke; tissue injury risk rises with delay.
- Prioritize Hypotheses: Immediate emergency escalation is highest priority.
- Generate Solutions: Notify nurse immediately, record onset time, keep resident safe, and prepare for urgent transfer.
- Take Action: Execute rapid report with objective findings and time details.
- Evaluate Outcomes: Resident reaches definitive treatment pathway without avoidable delay.
Related Concepts
- fall-prevention - Proactive risk reduction lowers emergency injury burden.
- choking-maneuver-and-airway-clearance - Airway obstruction response is a core emergency skill set.
- body-mechanics-and-safe-equipment-use - Safe lifting and transfer reduce fall and injury emergencies.
- documenting-and-reporting-data - Time-stamped objective documentation improves emergency continuity.
- communication-within-the-health-care-team - Clear escalation language supports rapid coordinated response.
Self-Check
- Which stroke finding in FAST requires immediate emergency escalation?
- What three details should be reported after a witnessed seizure?
- Why should a fallen resident usually not be moved before nurse assessment?