Parkinson’s Disease
Key Points
- Parkinson disease is a progressive movement disorder that can progress from mild unilateral symptoms to total ADL dependence.
- Core mechanism is dopamine depletion with relative acetylcholine excess in motor pathways.
- Basal-ganglia degeneration can involve both dopamine and norepinephrine pathways, contributing to autonomic instability.
- Current pharmacotherapy is symptomatic only; it does not stop neuronal degeneration.
- Cardinal motor features are resting tremor, rigidity, bradykinesia/akinesia, and postural instability.
- Autonomic and cognitive-behavioral symptoms can emerge as disease burden advances.
- Levodopa response is nutrition-sensitive: high-protein co-ingestion can reduce effect, while B-vitamin adequacy supports homocysteine-risk mitigation.
Pathophysiology
Parkinson disease reflects progressive dopaminergic neuron loss and decreased dopamine-mediated inhibition in motor-control pathways. As dopamine falls, relative cholinergic excitatory activity becomes functionally dominant, impairing coordinated voluntary movement.
Clinical motor symptoms usually become apparent after substantial dopamine depletion. Dopamine loss is also linked to autonomic changes such as orthostatic hypotension, drooling, and nocturia, which increase daily safety burden.
Pathologic alpha-synuclein aggregation (Lewy-body patterns) is associated with additional cognitive-behavioral changes in progressive disease.
Clinical Manifestations
- Resting tremor: Most common initial complaint; decreases with purposeful movement and may present as classic pill-rolling.
- Rigidity: Increased resistance to passive movement, often cogwheel quality, progressing to generalized stiffness and limited ADL function.
- Bradykinesia/Akinesia: Slowed or absent voluntary movement initiation, including difficulty rising from seated position.
- Postural instability and gait change: Forward-flexed posture with propulsive shuffling gait and high fall risk.
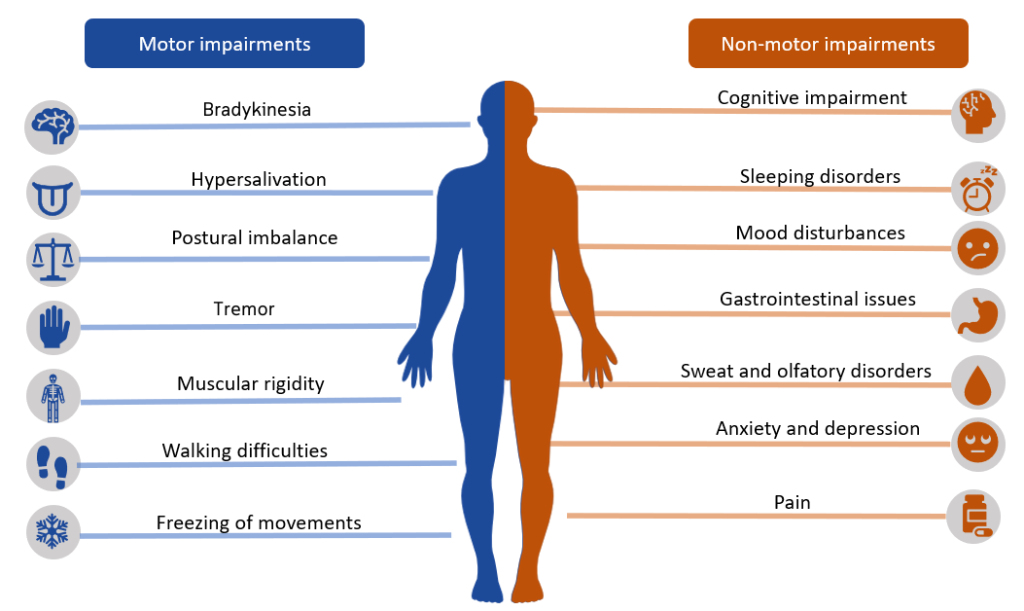 Illustration reference: OpenRN Health Alterations Ch.9.6.
Illustration reference: OpenRN Health Alterations Ch.9.6.
Progressive facial and bulbar muscle involvement can produce mask-like facies, dysarthria, swallowing difficulty, and aspiration/malnutrition risk. Later disease may also include psychosis or dementia-spectrum cognitive decline.
Classification
- Stage 1 (Initial): Unilateral limb involvement with mild tremor/weakness.
- Stage 2 (Mild): Bilateral involvement with resting tremor, bradykinesia, and mask-like facial expression.
- Stage 3 (Moderate): Postural instability, gait irregularity, and pill-rolling tremor.
- Stage 4 (Severe): Marked akinesia and rigidity with major functional impairment.
- Stage 5 (Total Dependence): Near-complete caregiver dependence for ADLs.
Nursing Assessment
NCLEX Focus
Distinguish chronic baseline parkinsonian findings from sudden new focal deficits that may indicate a separate acute neurologic emergency.
- Assess gradual progression pattern, symptom burden, and current stage-related functional limits.
- Assess cardinal symptoms: resting tremor, rigidity, bradykinesia/akinesia, and postural instability.
- Assess fall risk, transfer safety, and ADL dependence trend over time.
- Report changes in strength, gait, mobility, or cognition because these often indicate meaningful functional decline.
- Assess for autonomic symptoms (orthostasis, drooling, nocturia) and evolving cognitive/behavioral changes.
- Assess speech-volume change, swallowing safety, and aspiration warning signs as rigidity progresses.
- Assess for constipation, urinary retention, sexual dysfunction, sleep disturbance, depression, hallucinations, and impaired judgment/decision-making.
- Prioritize common nursing-diagnosis domains: impaired mobility, swallowing difficulty, confusion/memory change, communication impairment, fall risk, activity intolerance, and constipation.
Diagnostic Approach
There is no single confirmatory test for Parkinson disease. Diagnosis is primarily clinical and supported when at least two cardinal motor findings are present. Additional testing is used to exclude alternative neurologic causes:
- Blood tests to evaluate non-parkinsonian causes of symptoms.
- DAT scan/SPECT pathways in selected contexts to identify dopaminergic-system dysfunction.
- SPECT in selected contexts to identify reduced dopamine-producing neuron activity.
- CSF analysis that may show dopamine reduction patterns.
- MRI and PET to support differential assessment and rule out structural alternatives.
- CT imaging can help exclude other structural causes but does not confirm Parkinson disease directly.
Nursing Interventions
- Use a mobility and fall-prevention plan matched to current stage and gait instability.
- Keep assistive devices within reach and allow additional time to complete ADLs safely.
- Preserve independence by allowing extra time for ADLs while providing targeted assistive support.
- Coordinate early access to movement-disorder expertise and rehabilitation services when available.
- Address health-equity barriers that limit access to specialty, rehabilitation, and mental-health care.
- Reevaluate care goals over time for mobility, aspiration prevention, communication effectiveness, bowel function, and safety outcomes.
- Collaborate with PT/OT for ROM/stretching/activity plans, assistive-device training, and adaptive equipment to preserve ADL participation.
- Collaborate with SLP for dysarthria and dysphagia support, including swallow-muscle exercise and alternate communication modalities.
- When medication response declines, anticipate advanced-management discussions (for example stereotactic pallidotomy or deep-brain stimulation) and reinforce postoperative monitoring plans.
- Administer PD medications on schedule to maintain therapeutic consistency and monitor for orthostatic hypotension, confusion, and hallucinations.
- Implement immobility-prevention measures (pressure-injury prevention, bowel plan, contracture prevention) while preserving autonomy.
- Time activities for peak-function periods (often later morning) to reduce rushing and fatigue.
- Coordinate dietician input for dysphagia diets (for example soft foods/thickened liquids), nutrition supplements, and constipation-focused diet adjustments.
- Time levodopa administration about 30-60 minutes before meals when feasible and monitor for reduced efficacy when high-protein intake clusters around dosing.
Expected Outcomes
- Client remains free from serious fall or immobility complications.
- Nutrition and hydration remain adequate while aspiration events are prevented.
- Communication strategies are sufficient for care needs.
- Client and caregivers can describe symptom-management and coping strategies.
Health Teaching and Care Transitions
- Teach safe medication administration and early reporting of acute confusion, hallucinations, and severe orthostatic symptoms.
- Teach household fall-risk reduction (remove clutter/rugs, use assistive devices correctly).
- Reinforce symptom-management routines: fluids/fiber for constipation, sleep-hygiene habits, and strength-focused coping.
- Encourage caregiver use of support groups and Parkinson-specific community organizations.
- Engage case-management/social-work support for psychosocial planning, insurance/financial navigation, respite planning, and potential long-term-care transition.
Evaluation
Outcome evaluation is continuous and should be repeated at each reassessment, major diagnostic/laboratory update, and interdisciplinary/family care review. If outcomes are partially met or unmet, revise and reimplement the care plan.
Complication Risk
Progressing rigidity, gait disturbance, and swallowing decline increase risk for falls, aspiration, malnutrition, and caregiver strain.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| dopaminergic-therapy | Carbidopa/levodopa, dopamine agonist contexts | Monitor for symptom fluctuation, dyskinesia, orthostasis, and neuropsychiatric adverse effects. |
| MAO-B/MAOI contexts | Selegiline, rasagiline | Reinforce tyramine precautions and monitor for hypertensive or adverse neurologic effects. |
| Anticholinergic contexts | Benztropine, trihexyphenidyl | Monitor older adults for poor tolerance, urinary retention (especially with BPH), and increased intraocular-pressure risk. |
| COMT inhibitor contexts | Entacapone, tolcapone | Used with carbidopa/levodopa to prolong benefit duration; monitor response and adverse effects. |
| Dopamine-antagonist context | amantadine | Monitor for suicidality, edema/heart-failure worsening, and abrupt-withdrawal NMS-like risk. |
| Adenosine-pathway adjuncts | istradefylline contexts | May reduce “off” episodes in selected levodopa regimens; monitor dyskinesia and insomnia patterns. |
| Parkinson psychosis therapy | pimavanserin contexts | Used for hallucination/delusion pathways in selected cases; monitor QT-related and mental-status safety concerns. |
Levodopa-based regimens are most effective early in disease but may lose duration over time. Long-term treatment (often after 5-10 years) can produce dyskinesia and tolerance patterns requiring dose/frequency adjustment, regimen change, or closely monitored medication interruption in selected cases.
Clinical Judgment Application
Clinical Scenario
An older adult with Parkinson disease reports worsening shuffling gait, rising near-falls, and new dependence for dressing.
- Recognize Cues: Progressing motor dysfunction with increasing injury risk.
- Analyze Cues: Stage progression is reducing safe mobility and ADL capacity.
- Prioritize Hypotheses: Immediate safety stabilization and fall-risk reduction are priority.
- Generate Solutions: Strengthen transfer supervision, optimize assistive devices, and coordinate interdisciplinary reassessment.
- Take Action: Implement fall precautions and communicate functional decline to the care team.
- Evaluate Outcomes: Near-falls decrease and ADL plan is adjusted to preserve function.
Related Concepts
- neurological-system - Dopamine-pathway dysfunction in movement control.
- dopaminergic-therapy - Medication strategies for symptom control.
- common-neurological-disorders-recognition-and-priority-care - Pattern recognition and escalation context.
- fall-prevention - High-priority safety framework for gait and postural instability.
- caregiver-role-strain - Progressive dependence increases family-care burden.
Self-Check
- Which clinical findings indicate Parkinson progression rather than an acute stroke pattern?
- Why does dopamine depletion produce both motor and autonomic manifestations?
- Which care priorities best reduce injury as ADL dependence increases?