Traumatic Brain Injury
Key Points
- Traumatic brain injury can result from blunt force, acceleration-deceleration injury, or penetrating trauma.
- Presentation ranges from mild concussion to severe permanent disability or death.
- Red-flag findings include altered consciousness, focal deficits, unequal pupils, vomiting, and CSF leak signs.
- Imaging and concussion tools guide diagnosis and severity stratification.
- Management depends on cause/severity and can range from rest to urgent neurosurgical decompression.
- Temporal-side impact can produce delayed intracranial hematoma progression, so ongoing reassessment is essential even when initial findings appear mild.
- In veterans, repeated blast exposure can contribute to TBI burden with persistent sleep, hearing, pain, and GI symptom clusters that need longitudinal follow-up.
Pathophysiology
TBI occurs when external mechanical force disrupts brain tissue and normal neurologic function. Injury can be transient (as in mild concussion) or involve structural damage with bleeding, edema, and persistent neurologic impairment.
Secondary injury pathways, including swelling and increased intracranial pressure, can worsen outcomes after initial trauma.
TBI can be nonpenetrating (closed injury with intracranial acceleration-deceleration effects) or penetrating (skull breach with direct brain-tissue disruption). Primary injury occurs at impact; secondary injury may evolve over hours to weeks.
Classification
- Concussion: Mild TBI with temporary cognitive, behavioral, or neurologic dysfunction.
- Intracranial hematoma: Bleeding around or within brain compartments after vascular rupture.
- Skull fracture-associated injury: Bony cranial disruption with risk of underlying brain and vessel injury.
- Chronic traumatic encephalopathy (CTE): Delayed progressive neurologic disorder after repeated head-impact exposure.
- Military blast-exposure TBI domain: Repeated blast events can cause cumulative neurotrauma and prolonged multisystem sequelae.
Nursing Assessment
NCLEX Focus
Detect deterioration early through serial neurologic checks and escalation of red-flag findings.
- Assess level of consciousness and acute cognitive or behavior change.
- Assess for headache, blurred vision, unequal pupils, nausea/vomiting, photophobia, tinnitus, and focal deficits.
- In sports/recreation contexts, assess concussion warning cues needing immediate medical evaluation: vomiting, balance problems, fatigue/drowsiness, dazed/confused appearance, concentration or memory difficulty, emotional irritability, or personality change.
- Assess for clear fluid drainage from nose/ears as possible CSF leak signal.
- Assess injury mechanism and repeated-impact exposure history.
- Assess deployment and blast-exposure history in veterans when cognitive, sleep, hearing, or persistent post-concussive symptoms are reported.
- Assess mechanism details including seemingly minor rapid deceleration events (for example collision with fixed objects) because concussion can occur without obvious external trauma.
- Incorporate age-context risk clues during mechanism review because falls are a leading head-injury mechanism in young children, adolescents, and older adults.
- After lateral/temporal impact, monitor closely for evolving hematoma indicators because neurologic decline may be delayed.
Diagnostic and Monitoring Data
- Use standardized concussion-assessment tools for mild injury screening.
- Use CT/MRI when clinically indicated to evaluate structural injury, bleeding, and severity context.
- Use neuropsychological testing when needed to characterize concentration, memory, and executive-function deficits after trauma.
- Trend Glasgow Coma Scale GCS data closely; lower scores indicate more severe injury burden (for example below 8 signals severe consciousness impairment).
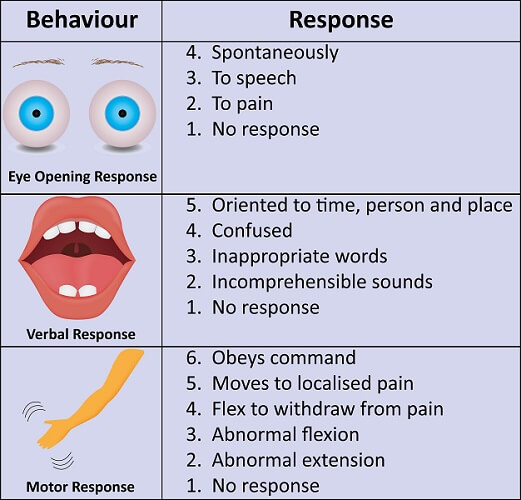 Illustration reference: OpenRN Health Alterations Ch.9.3.
Illustration reference: OpenRN Health Alterations Ch.9.3.
Nursing Interventions
- Implement frequent neurologic reassessment and immediate escalation for worsening signs.
- Support cause/severity-specific treatment plans: rest and symptom control in mild concussion patterns, including temporary cognitive/visual-load reduction (for example limiting reading/screen exposure) with graded return to activity.
- Escalate any suspected concussion for same-day provider or emergency evaluation rather than watchful delay.
- Prepare for neurosurgical pathways when severe injury causes pressure-related deterioration.
- In rising-ICP trajectories, support ordered head-of-bed elevation (about 30 degrees) with neutral neck alignment while emergency escalation is underway.
- Implement low-stimulation seizure-prevention measures when indicated (for example reduced light/noise and seizure-safety setup).
- In immediate first-aid response, prioritize responsiveness and breathing checks, emergency activation for unconsciousness/respiratory compromise, gentle bleeding control, and cervical-motion protection when head/neck injury is suspected.
- Reinforce prevention counseling (helmet and seat-belt use, high-risk activity protection).
- Include adolescent-focused injury prevention teaching when relevant: no texting/phone use while driving, speed-limit adherence, and consistent seat-belt/helmet use.
Rapid Neurologic Deterioration Risk
Worsening intracranial pathology can become life-threatening; delayed escalation increases permanent-deficit risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Symptom-directed analgesia (mild injury context) | Protocol-directed pain relievers | Use cautiously with ongoing neurologic reassessment. |
| Sedation/anesthesia support (severe injury context) | Procedure-specific | Coordinate with airway and ICP management strategies when surgical intervention is required. |
| Neuroprotection-support contexts | antiseizure, osmotic-diuretic, and selected coma-induction pathways by severity | Used in selected severe trajectories to limit secondary injury; requires high-acuity neuro-respiratory monitoring. |
Clinical Judgment Application
Clinical Scenario
A patient with head trauma develops worsening headache, repeated vomiting, and new unequal pupils.
- Recognize Cues: Progressing intracranial injury warning signs.
- Analyze Cues: Secondary neurologic deterioration is likely.
- Prioritize Hypotheses: Prevent herniation and permanent brain injury.
- Generate Solutions: Escalate urgently for emergent imaging and neurosurgical evaluation.
- Take Action: Activate emergency pathway and intensify neurologic monitoring.
- Evaluate Outcomes: Definitive intervention is delivered before irreversible decline.
Related Concepts
- neurological-diagnostic-testing-and-nursing-considerations - CT/MRI and neuro-monitoring principles.
- intracranial-hypertension-and-increased-intracranial-pressure - Pressure-deterioration recognition and stabilization priorities across neuro injuries.
- stroke - Differential diagnosis in acute focal neurologic deficits.
- common-neurological-disorders-recognition-and-priority-care - Pattern recognition and escalation across neurologic emergencies.
Self-Check
- Which symptoms most strongly suggest severe rather than mild TBI?
- Why are serial neuro checks critical after initial TBI stabilization?
- How do management priorities differ between concussion and severe TBI with mass effect?