Warfarin
Key Points
- Warfarin (Coumadin) is an oral anticoagulant that inhibits synthesis of vitamin K-dependent clotting factors II, VII, IX, and X.
- INR target range: 2.0–3.0 for most indications; 2.5–3.5 for mechanical heart valves — INR must be monitored regularly.
- Full anticoagulant effect is delayed 5–7 days after initiation; heparin bridge therapy is required in acute clotting events.
- Major risk: bleeding — ranging from minor bruising to fatal intracranial hemorrhage. INR >3.5 significantly elevates risk.
- Warfarin-associated acute kidney injury can occur; bleeding risk is higher in liver disease.
- Antidote: vitamin K (phytonadione) — fresh frozen plasma (FFP) for urgent reversal.
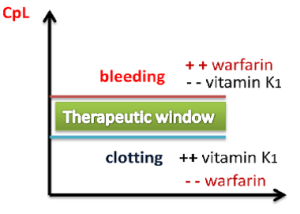 Illustration reference: OpenRN Nursing Pharmacology 2e Ch.1.10.
Illustration reference: OpenRN Nursing Pharmacology 2e Ch.1.10.
Mechanism of Action
Warfarin inhibits vitamin K epoxide reductase, blocking the regeneration of active vitamin K. Vitamin K is required for hepatic synthesis of clotting factors II, VII, IX, and X and anticoagulant proteins C and S. By reducing production of these factors, warfarin shifts the coagulation balance toward anticoagulation.
Onset of action: The anticoagulant effect is not immediate — existing clotting factors must be depleted. Full therapeutic effect typically requires 5–7 days. For this reason, when treating acute thromboembolism, heparin is initiated simultaneously and discontinued once INR reaches target range.
Indications
- Prevention and treatment of deep vein thrombosis (DVT) and pulmonary embolism (PE)
- Stroke prevention in atrial fibrillation
- Thromboembolism prophylaxis with mechanical heart valve replacement
- Reduction in recurrent MI risk and thromboembolic events post-myocardial infarction
INR Monitoring
| Indication | Therapeutic INR Range |
|---|---|
| DVT/PE prevention and treatment | 2.0–3.0 |
| Atrial fibrillation | 2.0–3.0 |
| Mechanical heart valves | 2.5–3.5 |
Monitoring frequency: Frequent during initiation and with any medication or lifestyle changes; may be reduced to monthly once stable. Point-of-care INR testing allows home monitoring for eligible clients.
Nursing Assessment
NCLEX Focus
Warfarin is a high-alert medication — it has the highest risk of serious patient harm among commonly used drugs. Before each dose, verify the current INR and check for signs of bleeding. INR below 2.0 = underanticoagulated (clotting risk); INR above 3.5 = overanticoagulated (bleeding risk).
Pre-administration assessment:
- Review current INR (obtain result before dose if newly initiated or dose-adjusted)
- Assess for active bleeding: blood in urine/stool, unusual bruising, prolonged bleeding from minor cuts
- Review all concurrent medications — warfarin has extensive drug interactions via cytochrome P450 (CYP2C9) metabolism
- Screen for pregnancy (warfarin is teratogenic; contraindicated in pregnancy except mechanical heart valves)
- Screen for major contraindication patterns: hemorrhagic tendencies/blood dyscrasias, recent or planned CNS/eye surgery, active GI/GU/respiratory tract bleeding, CNS hemorrhage, cerebral aneurysm/dissecting aorta, pericarditis/pericardial effusion, and bacterial endocarditis
Drug interactions that increase bleeding risk (↑ INR):
- Antibiotics (especially fluoroquinolones, metronidazole)
- NSAIDs, aspirin
- Amiodarone, statins, certain antifungals
- Tamoxifen and related coumarin-sensitive oncology pathways may potentiate anticoagulant effect and require close INR surveillance or regimen reconsideration
Drug interactions that reduce effectiveness (↓ INR):
- Rifampin, carbamazepine, barbiturates
Food interactions:
- High vitamin K foods (kale, spinach, broccoli, brussels sprouts, collard greens) oppose warfarin’s effect
- Dietary vitamin K intake must be consistent — sudden increases or decreases in intake significantly alter INR
- Practical intake anchor: many adult teaching plans use about 90 mcg/day vitamin K for women and about 120 mcg/day for men; consistency is more important than strict avoidance.
Nursing Interventions
Safety and monitoring:
- Monitor INR as ordered; hold dose and notify provider if INR >3.5 or signs of major bleeding
- Implement bleeding precautions: soft-bristle toothbrush, electric razor, avoid IM injections
- Avoid activities with high injury risk
Reversal:
- Vitamin K (phytonadione) — primary antidote; oral or IV administration (IV causes faster reversal)
- Fresh frozen plasma (FFP) — for urgent/emergent reversal when rapid factor replacement is needed
- Prothrombin complex concentrate (PCC) — used in severe bleeding for faster reversal than FFP
Boxed Warning: Fatal Bleeding
Warfarin can cause major or fatal bleeding. Monitor INR regularly. Patients must be educated on signs of bleeding (red or dark urine, black tarry stools, unexplained bruising, prolonged nosebleeds) and instructed to report immediately.
Patient education:
- Take at the same time each day; never double a missed dose
- Maintain consistent (not zero) vitamin K dietary intake — avoid excessive amounts of green leafy vegetables; do not suddenly stop eating them
- Keep high-vitamin K food patterns steady across weeks (for example leafy greens, Brussels sprouts, broccoli, asparagus, and green tea) to reduce INR instability.
- Avoid alcohol, cranberry juice, and grapefruit — increase bleeding risk
- Carry medical alert identification stating warfarin use
- Recognize that tablet strengths may use different colors; verify each dose against the current prescription and do not interchange strengths without instruction
- Inform all providers and dentists of warfarin therapy before any procedure or new medication
- Report frequent falls to the provider due to intracranial bleeding risk
- Report immediately: nosebleeds, blood in urine/stool, prolonged cut bleeding, headache, dizziness, or sudden weakness (signs of intracranial bleeding)
Related Concepts
- hemostasis-coagulation-and-fibrinolysis — Coagulation cascade and vitamin K-dependent factors blocked by warfarin.
- anticoagulants — Warfarin in context of anticoagulant drug class including heparins and DOACs.
- thrombocytopenia-bleeding-risk-and-management — Bleeding risk assessment in anticoagulated patients.
- blood-transfusion-verification-initiation-and-reaction-response — FFP transfusion for emergency warfarin reversal.
- high-alert-medications — Warfarin as a high-alert medication requiring double-checks and systematic monitoring.
- medication-side-effect-surveillance-and-reporting — INR monitoring and bleeding surveillance as adverse effect tracking.
Self-Check
- A client is started on warfarin for DVT. Why is heparin also initiated on day 1, and when is it discontinued?
- A client taking warfarin begins a course of metronidazole for a GI infection. What would you anticipate will happen to their INR and why?
- A client reports eating large amounts of kale and spinach this week. Their INR is 1.6. What nursing action and education is appropriate?