Assisting With Ambulation
Key Points
- Ambulation preserves bone loading, joint mobility, and functional independence.
- Safe walking assistance requires care-plan review, nonskid footwear, and gait-belt support when indicated.
- CNA positioning should be slightly behind and on the weaker side to provide controlled support.
- Matching adaptive devices (wheelchair, walker, cane) to current deficits can restore mobility and improve participation in self-care activities.
- Nurse-driven early mobility protocols in ICU/post-op settings support baseline function, lower delirium burden, and shorter hospital stay when readiness screening is used.
Pathophysiology
Walking provides weight-bearing stimulus that supports musculoskeletal maintenance and circulation. Inactivity rapidly reduces strength, balance, and endurance, increasing fall risk and dependence.
During assisted ambulation, postural instability and orthostatic symptoms may emerge, especially in frail residents or those with cardiovascular medication effects. Incorrect assistive-device use can worsen imbalance rather than improve safety.
Consistent cueing and correct support technique lower fall risk while preserving resident mobility capacity.
Classification
- Independent ambulation: Walks without hands-on support.
- Assisted ambulation: One or two assistants with gait belt.
- Device-assisted ambulation: Cane, standard walker, 2-wheeled walker, or 4-wheeled walker per therapy recommendation; standard/2-wheeled walkers usually provide slower, higher-support gait than 4-wheeled walkers.
- Cane-assisted ambulation: Single-point or quad cane support; quad canes provide a wider base of support for selected balance deficits.
- Crutch-assisted ambulation: Axillary, forearm/elbow, or gutter crutches selected by weight-bearing status and upper-extremity capability.
- Knee-walker ambulation: Wheeled knee-scooter option for selected lower-limb injuries requiring offloading with preserved standing balance.
- Guarded ambulation: Assistant positioned at weak side with wheelchair follow support when needed.
Nursing Assessment
NCLEX Focus
Priority questions ask which side to assist, which device pattern to cue, and what to do when weakness or dizziness develops.
- Verify prescribed ambulation status and assistive-device type before mobilization.
- Assess resident readiness: footwear, dizziness, pain, and fatigue.
- Confirm resident is cooperative, can bear weight as ordered, has sufficient trunk control, and can transition from sitting to standing with expected assist level.
- Verify assistive-device fit and safety:
- cane height aligned to wrist-crease level with about 15-degree comfortable elbow flexion
- axillary crutch clearance about two fingers below axilla to reduce nerve-compression risk
- wrist/hand support needs that may require gutter or forearm adaptations
- walker brake-function checks for 4-wheeled models before standing and during stops
- Assess adoption barriers to assistive-device use, including knowledge gaps, safety fears, stigma, affordability, home-space limits, and language/literacy mismatch.
- In protocol-driven units, screen readiness criteria before ambulation attempts (neurologic response to verbal stimulation plus respiratory/circulatory stability checks).
- Identify weaker side and position support accordingly.
- Observe gait quality (purposeful stepping vs shuffling) and tolerance distance.
Nursing Interventions
- Assist resident to dangle before standing, then reassess dizziness.
- Ensure nonskid footwear and correct device setup before walking.
- If dizziness/light-headedness appears before first steps, assist resident back to seated position and delay ambulation until symptoms resolve.
- For cane use, place cane on stronger side and cue sequence with weaker leg support.
- Cue cane movement with the affected/weak limb so load is shared and balance improves.
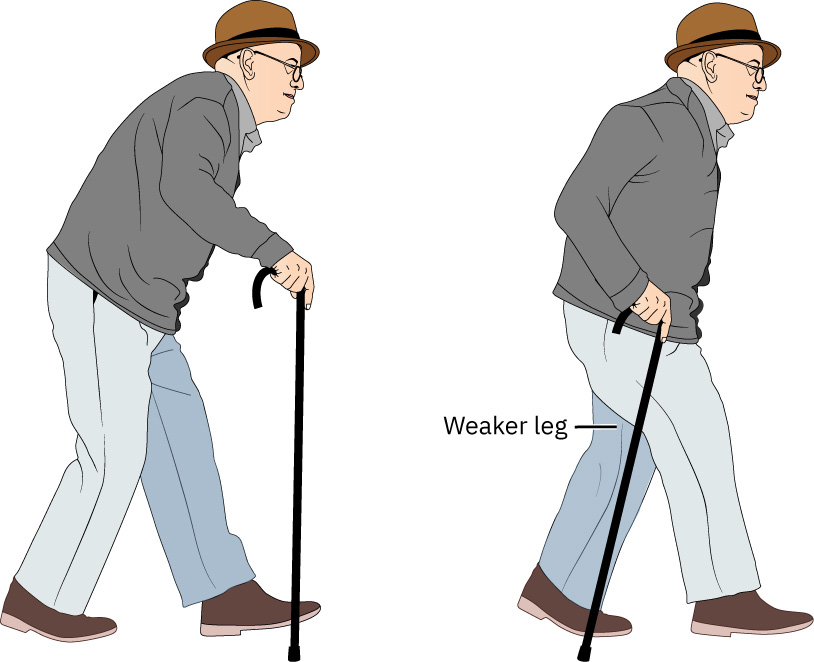 Illustration reference: OpenStax Clinical Nursing Skills Ch.9.
Illustration reference: OpenStax Clinical Nursing Skills Ch.9. - For crutch gait training, cue coordinated advancement and controlled step-through with the stronger limb while respecting ordered weight-bearing limits.
- Walk at resident’s side and slightly behind with secure gait-belt handhold (fingertips up under belt) and cue upright posture, forward gaze, and purposeful non-shuffling steps.
- Monitor vital signs and activity response before, during, and after ambulation (for example heart rate, blood pressure, dyspnea pattern, and skin color change).
- For clients with exertional hypoxemia risk, apply ordered oxygen support before ambulation, reassess early walk SpO2, and titrate only within RN order/protocol limits to maintain target saturation.
- During ambulation, periodically reassess for dizziness, weakness, and fatigue; limit distance to current tolerance.
- If sustained walking is not tolerated, transition to the prescribed wheelchair or alternate assistive-device plan to maintain safe mobility and self-care participation.
- Escalate to RN/provider if oxygen saturation remains below target or required oxygen flow exceeds ordered limits during activity.
- Use wheelchair follow support for residents with intermittent weakness risk.
- For 4-wheeled walkers, remind patients to lock brakes before stationary tasks or sitting to reduce roll-away fall risk.
- Deliver culturally and linguistically appropriate device teaching, and use return demonstration to confirm safe use and reduce fear-based nonadherence.
- In early mobility protocols, coordinate with RN/PT and other team members to match ambulation intensity and frequency to current clinical criteria.
- When returning to chair/bed, cue knees to contact seat edge before controlled descent while maintaining gait-belt support.
- If returning to bed, place bed in lowest safe position, apply ordered side-rail setup, and keep call light in reach.
- Document ambulation distance and tolerance response after each assisted-walk event.
- If resident begins to fall, do not try to catch abruptly; widen base, support at gait belt/hip, lower resident in a controlled descent while protecting the head.
- After a witnessed or unwitnessed fall, do not move resident until nurse assessment; then use ordered lift-based transfer method for return to bed/chair.
Unsupported Gait Risk
Ambulating residents without prescribed support method or proper assistant position can lead to sudden loss of balance and injury.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| antihypertensives | Blood-pressure management therapies | Monitor for postural dizziness during standing and ambulation transitions. |
| sedatives | Sleep/anxiety medications | Sedation and slowed reflexes require closer guarding and shorter supervised ambulation intervals. |
Clinical Judgment Application
Clinical Scenario
A resident using a walker starts shuffling and reports “my legs feel weak” halfway to the dining area.
- Recognize Cues: Fatigue, altered gait pattern, and reduced lower-extremity control.
- Analyze Cues: Current ambulation demand exceeds immediate tolerance.
- Prioritize Hypotheses: Primary priority is preventing fall while preserving dignity.
- Generate Solutions: Slow pace, reinforce upright posture, provide gait-belt support, and bring wheelchair for seated rest.
- Take Action: Transition resident safely to seated support and report tolerance change.
- Evaluate Outcomes: Resident remains injury-free and ambulation plan is adjusted.
Related Concepts
- assisting-clients-to-transfer - Safe transfer setup is prerequisite to safe ambulation starts and stops.
- moving-and-positioning-clients - Mobility and positioning plans are integrated pressure-injury prevention strategies.
- fall-prevention - Ambulation support choices directly affect fall risk.
- promoting-joint-mobility-and-activity - Walking is a core daily activity for preserving function.
- body-mechanics-and-safe-equipment-use - Assistant stance and grip technique reduce caregiver injury.
Self-Check
- Where should the assistant stand when the resident has one weaker side?
- Why should residents dangle before starting assisted ambulation?
- What signs indicate ambulation should pause and support level should increase?