Coronary Artery Disease
Key Points
- Coronary artery disease (CAD) is caused by atherosclerotic plaque narrowing coronary arteries and reducing oxygenated myocardial blood flow.
- Stable angina is predictable and generally relieved by rest or nitroglycerin, whereas unstable angina is an acute coronary syndrome (ACS) warning pattern.
- ACS ranges from unstable angina to myocardial infarction (MI) and requires urgent escalation.
- ECG and troponin trends are central for ischemia/injury/infarction identification and rapid treatment decisions.
- Women may present with atypical ischemic symptom patterns (for example neck, jaw, shoulder, upper-back, or abdominal discomfort) and can have less classic chest-radiation findings.
- Core interventions include oxygen when indicated, antiplatelet therapy, anti-ischemic therapy, and revascularization when occlusion is significant.
- Safety teaching includes nitroglycerin self-administration steps, storage, side effects, and when to call 911.
- Coronary disease burden rises with age; prevalence bands are about 7.1% (age 45-65), 10.9% (age 45+), and 17% (age 65+).
- Social risk clusters (lower educational access, physical inactivity, tobacco exposure, and low surveillance access) can worsen CAD event burden.
Pathophysiology
CAD develops when atherosclerotic plaque progressively narrows coronary arteries. Reduced lumen diameter limits oxygenated blood delivery to cardiac muscle, especially during exertion when myocardial oxygen demand rises. Diet patterns high in saturated/trans fats and cholesterol can maintain elevated LDL and accelerate plaque deposition in coronary vessels.
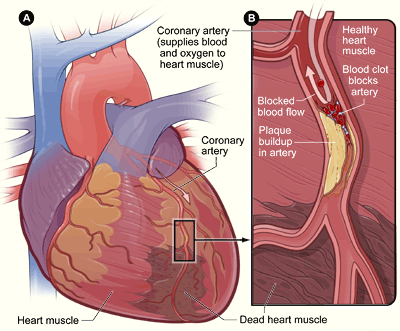 Illustration reference: OpenRN Health Alterations Ch.5.7.
Illustration reference: OpenRN Health Alterations Ch.5.7.
Ischemia causes angina and may be reversible if oxygen supply is restored quickly. CAD typically progresses along a continuum from stable angina to unstable angina (ACS context), and when obstruction persists, myocardial injury can advance to infarction with irreversible tissue death. Major vessel territory context guides ischemic-pattern interpretation: the right coronary artery supports right-ventricular and sinoatrial-node perfusion, the left circumflex supplies left-atrial/lateral regions, and the LAD and left-main pathways support high-demand anterior/septal-left-ventricular territories.
Classification
- Stable angina: Chronic, generally predictable chest pain from partial narrowing, typically improving with rest or nitroglycerin.
- Unstable angina: Worsening or sudden ischemic pain pattern that is less responsive to rest/nitroglycerin and signals ACS risk.
- Acute coronary syndrome (ACS): Sudden reduction in myocardial oxygenated flow spectrum from unstable angina to MI.
- Myocardial infarction (MI): Acute coronary occlusion with myocardial necrosis.
Nursing Assessment
NCLEX Focus
Prioritize rapid differentiation of stable versus unstable symptoms, immediate MI cue recognition, and timely escalation for definitive care.
- Assess CAD risk factors, including modifiable factors (hypertension, dyslipidemia, smoking, obesity, inactivity, high-risk diet, chronic stress, excess alcohol) and nonmodifiable factors (age, family history/genetics, sex-related risk trends).
- In risk counseling, clarify lipid interpretation anchors: LDL is atherogenic (“bad”) cholesterol, HDL is relatively protective (“good”), and rising triglycerides increase overall cardiometabolic burden.
- Use adult trend interpretation for risk communication when available (for example total cholesterol desirable <200 mg/dL, LDL desirable <100 mg/dL, HDL low-risk support >60 mg/dL, and triglycerides desirable <150 mg/dL).
- Include social-determinant screening (education access, activity environment, and ongoing disease-surveillance access) because these factors influence CAD and MI outcomes.
- Assess chest pain pattern (provoking factors, duration, intensity, response to rest/nitroglycerin, and symptom progression).
- Assess for MI warning signs such as persistent chest pressure, dyspnea, diaphoresis, nausea, and anxiety.
- Assess for atypical ischemic symptoms, especially in women (for example neck, jaw, shoulder, upper-back, abdominal discomfort, or GI-upset presentation without classic chest-radiation pattern).
- Recognize higher post-MI risk in clients with major comorbidity burden (for example diabetes, CKD, COPD, cerebrovascular disease, and peripheral arterial disease) and escalate early for subtle deterioration.
- Obtain and trend stat ECG for ischemic/injury patterns and monitor for dynamic changes.
- In suspected MI, obtain rapid baseline perfusion data (radial/dorsalis pedis pulses, capillary refill, skin color, oxygen saturation) before invasive revascularization decisions.
- Monitor troponin trends when MI is suspected because elevated troponin supports myocardial cell death.
- Use serial biomarker timing to refine MI interpretation: troponin I commonly rises within about 2-6 hours, often has an early peak around 15-24 hours, and may show a later secondary peak around 60-80 hours; CK-MB often rises within about 4-6 hours, peaks near 24 hours, and usually normalizes by about 72 hours.
- In many emergency pathways, serial troponins are repeated every about 6-8 hours for three total measurements when initial testing is nondiagnostic.
- Recognize CK-MB is less cardiac-specific than troponin and may rise with skeletal-muscle injury or recent surgery.
- Monitor blood-glucose trends during acute MI because stress hyperglycemia is associated with higher complication and mortality risk.
- Escalate unstable angina or suspected ACS immediately to prevent infarction progression.
ECG and Biomarker Pattern Cues
- Ischemia: ST-segment depression can indicate myocardial ischemia.
- Injury progression: ST-segment elevation can indicate acute myocardial injury pattern requiring urgent reperfusion evaluation.
- Infarction evidence: Q-wave change with elevated troponin supports infarcted tissue.
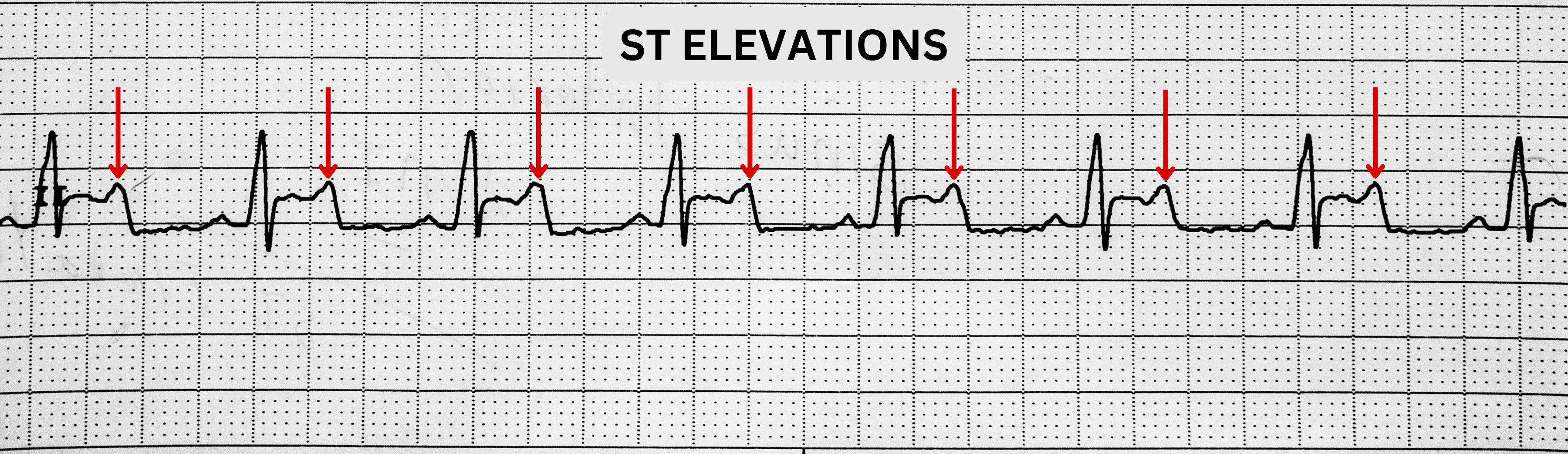 Illustration reference: OpenRN Health Alterations Ch.5.7.
Illustration reference: OpenRN Health Alterations Ch.5.7.
Nursing Interventions
- Initiate urgent ACS workflow and notify provider/activate emergency pathway per protocol.
- Record exact chest-pain onset time during suspected MI because reperfusion delay increases infarct size and protocolized transfer timing.
- Administer oxygen when SpO2 is less than 92% (or per agency protocol) to optimize myocardial oxygenation.
- Administer nitroglycerin as ordered to reduce ischemic pain and improve coronary perfusion.
- Administer antiplatelet therapy as ordered (for example, aspirin and clopidogrel) to reduce clot propagation risk.
- Support adjunct therapies as ordered, such as beta-blockers (to lower myocardial oxygen demand) and carefully selected analgesia/anxiolysis when appropriate.
- Recognize that morphine may be prescribed for refractory discomfort but is no longer first-line because of higher risk of adverse outcomes.
- Use continuous telemetry and frequent hemodynamic reassessment during acute-ischemia phases; support bed rest and a low-stimulation environment to limit oxygen demand.
- Prepare for or coordinate revascularization (cardiac catheterization, stenting/PCI, or CABG) when occlusion severity requires intervention.
- Support rapid reperfusion workflow in STEMI-equivalent presentations; chapter guidance emphasizes emergency activation targeting about a 90-minute angioplasty window.
- After femoral-access angiography, maintain ordered flat bedrest (commonly about 4-6 hours) and monitor puncture site and distal perfusion for bleeding or vascular compromise.
- For coronary angiography education, explain key procedural risks (bleeding, dysrhythmia, and embolic-clot dislodgement) and reinforce close postprocedure monitoring.
- If multivessel obstruction is present, anticipate CABG planning; graft options often include saphenous-vein harvest with single-to-quadruple bypass patterns based on disease extent.
- Reinforce post-MI targets during stabilization and discharge planning: SpO2 above 92%, hemodynamic stability, chest-pain control, graded activity with rest periods, medication adherence, and early cardiac-rehabilitation follow-up.
- Support protocol-directed glycemic management in acute MI to reduce arrhythmia, heart-failure, and recurrent-ischemia risk.
- Reinforce discharge and transition teaching, including lifestyle modification, medication adherence, follow-up labs, and referral to cardiac rehabilitation when indicated.
Lifestyle and Safety Teaching
- Teach a heart-healthy plan: reduced saturated/trans fat and sodium intake, weight optimization, smoking cessation, and regular physical activity.
- Reinforce activity targets when appropriate: adults about 150 minutes of moderate activity weekly (for example, brisk walking), with individualized progression.
- Teach alcohol moderation limits (commonly no more than two drinks/day for men and one drink/day for women) unless stricter limits are prescribed.
- Integrate mental-health support and stress-management strategies; refer to support groups or counseling when anxiety/depression interferes with adherence.
- Teach nitroglycerin safety: sit before sublingual dosing, use one tablet every five minutes for up to three doses, and store tablets in the original light-protected container.
- Teach expected effects and side effects (often relief in 1-2 minutes; possible headache, dizziness, flushing, or hypotension) and instruct immediate 911 activation for persistent or worsening chest pain.
Ongoing Evaluation
- Reevaluate outcomes after each intervention cycle, after new laboratory/diagnostic data, and after interprofessional care-plan discussions.
- If outcomes are unmet or only partially met within target time frames, revise the care plan and intervention priorities.
Time-Critical ACS Risk
Unstable angina can rapidly progress to myocardial infarction; delays in recognition and treatment increase irreversible myocardial damage risk.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Antiplatelet therapy | aspirin, clopidogrel | Reduce platelet aggregation and clot extension in CAD/ACS pathways. |
| Nitrate therapy | nitroglycerin, isosorbide | Dilate vessels, reduce ischemic pain, and require hypotension/symptom monitoring. |
| Beta-blocker therapy | class-based ACS use | Lower heart rate and contractility to decrease myocardial oxygen demand. |
| Antihypertensive therapy | ACE inhibitor or calcium blocker use | Reduce pressure load and myocardial strain; monitor blood pressure trends and tolerance. |
| Antiarrhythmic-related use | beta-blocker or calcium blocker use | Support rhythm control when dysrhythmia coexists with CAD/ACS; monitor rhythm and hemodynamic effect. |
| Thrombolytic therapy | class-based acute MI use | Consider in clot-occlusion pathways per protocol; monitor bleeding risk and reperfusion response. |
| Cholesterol-lowering therapy | statin-class prevention | Reduce atherosclerotic progression risk as part of long-term management. |
Clinical Judgment Application
Clinical Scenario
A patient with known CAD develops chest pain at rest that persists beyond 5 minutes and only partially improves after nitroglycerin.
- Recognize Cues: Rest pain with incomplete nitroglycerin response suggests unstable angina/ACS.
- Analyze Cues: Risk of imminent MI is high if perfusion is not restored quickly.
- Prioritize Hypotheses: Time-critical coronary occlusion progression is the immediate threat.
- Generate Solutions: Trigger ACS protocol, obtain ECG/troponin, and begin ordered medical therapy.
- Take Action: Escalate urgently, administer time-sensitive interventions, and prepare for possible revascularization.
- Evaluate Outcomes: Pain/perfusion improve and diagnostic trends guide definitive treatment.
Related Concepts
- hypertension-assessment-and-management - Hypertension accelerates atherosclerotic vascular injury and CAD progression.
- cardiovascular-and-peripheral-vascular-nursing-assessment - Structured assessment supports early ACS recognition and escalation.
- cardiac-rehabilitation-across-care-transitions - Post-event rehabilitation reduces recurrence risk and improves function.
- cardiovascular-system - Core cardiovascular physiology underpins CAD and MI pathophysiology.
- peripheral-vascular-system-and-insufficiency-patterns - Shared atherosclerotic mechanisms affect both coronary and peripheral circulation.
Self-Check
- Which assessment findings distinguish stable angina from unstable angina?
- How do ST-segment and troponin trends help differentiate ischemia, injury, and infarction?
- Why must clients be taught to call 911 after persistent chest pain despite nitroglycerin use?