Pneumonia
Key Points
- Pneumonia: acute infection causing inflammation of the alveoli → alveoli fill with fluid/purulent material → impaired gas exchange
- CAP remains a major mortality burden (eighth leading cause of death in the United States; high global burden).
- Highest risk: Adults >65 years, infants/young children, COPD, immunocompromise
- Priority assessments: SpO2, respiratory rate, sputum characteristics, mental status changes
- Diagnostic: Chest X-ray (consolidation) + CBC (elevated WBC) + sputum culture (guide antibiotic choice)
- Target SpO2: >92% — oxygen therapy titrated to maintain this level
- CURB-65 supports admission and ICU triage decisions in CAP.
- VAP prevention: HOB elevated 30–45°, oral hygiene every 2–4 hours, daily sedation vacation
Pathophysiology
Pneumonia is caused by microorganism invasion of the alveoli → inflammatory response → alveolar filling with fluid and purulent exudate → impaired gas exchange → hypoxia.
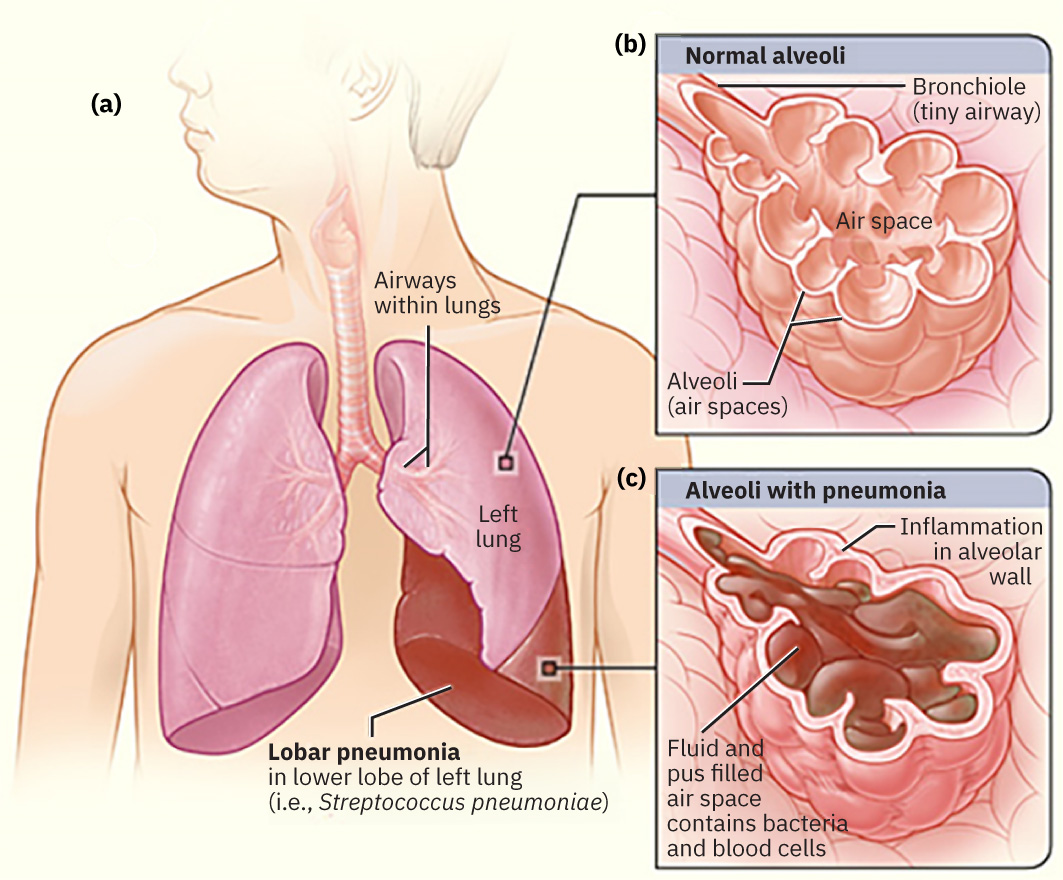 Illustration reference: OpenStax Medical-Surgical Nursing Ch.11.7.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.11.7.
Hospitalized pneumonia carries meaningful mortality risk, so early recognition and escalation are essential.
Common causative organisms:
- Bacteria: Streptococcus pneumoniae (most common), Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus, group A streptococci, aerobic gram-negative organisms (for example Klebsiella and Escherichia coli), Legionella, Mycoplasma pneumoniae, and Chlamydia species
- Viruses: Influenza A/B, SARS-CoV-2 and other coronaviruses, rhinovirus, parainfluenza, adenovirus, RSV, human metapneumovirus, and human bocavirus
- Fungi: Blastomyces, Histoplasma, Coccidioides, and selected opportunistic pathogens in immunocompromised hosts
Classification of Pneumonia
| Type | Definition | Key Considerations |
|---|---|---|
| CAP (Community-Acquired) | Acquired outside healthcare settings | Most common; outpatient or hospitalized treatment |
| HAP (Hospital-Acquired) | Onset ≥48 hours after hospital admission | Often caused by drug-resistant organisms |
| VAP (Ventilator-Associated) | Occurring after intubation and mechanical ventilation | High mortality risk; requires aggressive prevention |
| aspiration-pneumonia (Aspiration Pneumonia) | Inhalation of food, vomit, saliva, or medications | Risk: dysphagia (dysphagia), impaired gag reflex, oversedation, alcohol/drug use |
Common HAP/VAP organisms include Pseudomonas aeruginosa, Escherichia coli, Staphylococcus aureus, Enterobacter, and Acinetobacter.
Risk Factors and Severity Context
- Older age increases hospitalization risk; adults over 65 are at markedly increased CAP admission risk.
- Chronic lung disease, especially COPD, is a major risk factor for pneumonia-related hospitalization.
- Immunocompromise increases severity risk, including fungal pneumonia susceptibility.
- Aspiration-prone states (dysphagia, anesthesia, alcohol or drug effects, neurologic disease) raise pneumonia risk.
- Heavy alcohol use, opioid exposure, and smoking increase pneumonia risk.
- Socioeconomic and environmental exposure factors (poverty, crowded housing/shelters/prisons, inhalational toxin exposure) increase CAP risk and poor outcomes.
Clinical Manifestations
| Body System | Signs and Symptoms |
|---|---|
| Respiratory | Cough (nonproductive or productive of purulent sputum), dyspnea, tachypnea, pleuritic chest pain, fine crackles on auscultation, ↓ SpO2 |
| Cardiovascular | Tachycardia |
| Neurological | New onset confusion or altered mental status (especially older adults) |
| General | Fever, shaking chills (especially high fever), malaise, fatigue, weight loss |
| Musculoskeletal | Muscle aches and joint pain (common with viral pneumonia) |
| Integumentary | Diaphoresis, cyanosis (severe hypoxia) |
Sputum in bacterial pneumonia is often purulent or blood-tinged. Viral-pattern sputum may be watery, though mixed mucus or pus can still be seen.
Altered Mental Status in Pneumonia
New onset confusion or altered mental status — especially in older adults — may be the first and only symptom of pneumonia. Always assess for respiratory infection when mental status changes acutely in elderly patients.
Diagnostic Tests
Initial Assessment:
| Test | Finding in Pneumonia |
|---|---|
| Chest X-ray | Consolidation — areas of opacification (fluid/exudate in alveoli) |
| CBC | Elevated WBC (leukocytosis) → indicates infection |
| Sputum culture | Identifies causative organism → guides antibiotic selection |
| Pulse oximetry | ↓ SpO2 — severity indicator |
| CURB-65 score | Supports outpatient vs. admission vs. ICU triage |
Additional Testing for Hospitalized/Severe Cases:
- ABG: Assess PaO2, PaCO2, pH — determines severity of hypoxemia/hypercapnia
- Blood cultures: Determine if bacteremia (systemic spread) has occurred
- CT scan: Detailed lung imaging when diagnosis uncertain
- Bronchoscopy: Direct visualization; sample collection when cause unclear
- Pleural fluid culture (thoracentesis): If pleural effusion present
- Urinary antigen testing: Useful in selected pathogens such as suspected Legionella
- CRP/procalcitonin: Supports bacterial-versus-viral pattern differentiation
- Lactate: Helps risk-stratify possible septic pneumonia
Medical Management
Medication Therapy
| Category | Use |
|---|---|
| Antibiotics | Bacterial pneumonia — choice based on type (CAP vs. HAP/VAP) and culture results; may adjust after sensitivity results |
| Antivirals | Viral pneumonia (e.g., oseltamivir for influenza); antibiotics are not effective for viral-only causes |
| Antifungals | Fungal pneumonia (e.g., fluconazole, trimethoprim-sulfamethoxazole for PCP) |
| Bronchodilators | Albuterol — relieves bronchoconstriction, especially in COPD/asthma patients |
| Corticosteroids | Reduce severe airway inflammation |
| Antipyretics | Acetaminophen or ibuprofen for fever and discomfort |
Respiratory Support
- Supplemental oxygen: Titrate to maintain SpO2 >92%
- Incentive spirometry: Prevents atelectasis — instruct to use every 1–2 hours while awake
- Chest physiotherapy: Postural drainage and percussion — assists in clearing secretions
- BiPAP/CPAP: Non-invasive positive pressure ventilation for moderate-severe respiratory failure
- Mechanical ventilation: Severe cases requiring intubation
- Pleural procedures for pleural effusion: Thoracentesis and, when indicated, chest tube insertion to support lung re-expansion
Fluid Management
- Encourage oral fluids to thin secretions, with a practical target of about 2 liters/day unless fluid restriction is ordered
- IV fluids for high fever, poor oral intake, or dysphagia
Nursing Interventions
Priority Nursing Actions
Airway Clearance:
- Encourage coughing and deep breathing exercises hourly while awake
- Suction if patient cannot clear secretions independently
- Administer mucolytics/expectorants as ordered
- Positioning — upright (HOB 30–45°) to maximize lung expansion
- If aspiration risk is present, maintain NPO until a trained provider or SLP completes an evidence-based swallow screen.
Oxygenation:
- Monitor SpO2 continuously; maintain >92%
- Apply oxygen per orders; titrate to SpO2 target
- Assess respiratory rate, depth, and lung sounds every 4 hours
- Monitor ABG results as ordered
Infection Control:
- Hand hygiene before and after all patient contact
- Appropriate PPE and transmission-based precautions according to the suspected/confirmed organism
- Collect sputum culture BEFORE first antibiotic dose
VAP Prevention Bundle (for ventilated patients):
- HOB elevation 30–45°
- Oral hygiene every 2–4 hours with antiseptic
- Daily sedation vacation to assess readiness for extubation
- Deep vein thrombosis (DVT) prophylaxis
- Peptic ulcer disease prophylaxis
Patient Education
- Complete full course of antibiotics — even when feeling better
- Vaccination: Keep influenza vaccination current and follow pneumococcal vaccine recommendations, especially for at-risk adults and all adults age 65 or older
- Smoking cessation — smoking is major risk factor
- Oral hygiene to reduce aspiration risk
- Return precautions: worsening dyspnea, coughing up blood, fever >101°F (38.3°C)
Severity-Guided Antimicrobial Strategy
- CAP with CURB-65 0-1: Outpatient-leaning therapy; common options include macrolide or doxycycline when major comorbidity burden is low, with broader regimens when significant comorbid risk is present.
- CAP with CURB-65 2-3: Inpatient-level therapy is commonly recommended, often using broader dual-class coverage.
- CAP with CURB-65 4-5: ICU-level management with broad coverage is typically required.
- HAP/VAP: Broad-spectrum regimens are commonly used initially, then narrowed once microbiology and resistance data are available.
Evaluation and Care Plan Revision
- Reevaluate outcomes after interventions, new lab/diagnostic results, and interprofessional care-plan discussions
- Determine whether expected outcomes are met, partially met, or not met within the planned timeframe
- Revise the nursing care plan when outcomes are partially met or not met
CURB-65 Quick Triage
- Confusion: 1 point
- Uremia (BUN >20 mg/dL): 1 point
- Respiratory rate >=30/min: 1 point
- Blood pressure (SBP <90 mmHg or DBP <60 mmHg): 1 point
- Age >=65 years: 1 point
- Score
0-1: often outpatient management - Score
2-3: hospital admission generally recommended - Score
4-5: ICU-level care typically recommended
Related Concepts
- respiratory-system — Anatomy of the alveoli and lung lobes
- oxygen-therapy — Oxygen delivery devices and SpO2 monitoring
- respiratory-failure — Progression to respiratory failure in severe pneumonia
- antibiotics — Antibiotic selection for pneumonia
- bronchodilators — Bronchodilator therapy in pneumonia with obstructive disease
- sepsis — Pneumonia as leading cause of sepsis
- evidence-based-respiratory-care — Respiratory care protocols
Self-Check
- An 80-year-old patient with pneumonia is oriented x1 (knows name only), febrile at 101.8°F, and has fine crackles bilaterally. SpO2 is 89% on room air. What is the priority nursing intervention, and what SpO2 target should the nurse maintain?
- A nurse is about to administer the first dose of antibiotics for a patient diagnosed with community-acquired pneumonia. What should be done before administering the antibiotic, and why?
- A ventilated patient in the ICU develops a new fever, purulent sputum, and chest X-ray showing new infiltrate 3 days after intubation. What type of pneumonia is suspected, and what prevention measures should have been implemented?