Acute Respiratory Distress Syndrome
Key Points
- Acute respiratory distress syndrome (ARDS) is the most severe form of acute respiratory failure, with nearly 40% mortality.
- ARDS results from widespread lung inflammation causing fluid accumulation in the alveoli — severely impairing gas exchange.
- Diagnostic criteria: acute onset within 1 week, bilateral lung infiltrates on chest X-ray (noncardiac origin), PaO₂/FiO₂ ratio <300 mmHg.
- Hallmark assessment finding: hypoxemia that does not improve with supplemental oxygen (refractory hypoxemia).
- Treatment priorities: mechanical ventilation with lung-protective strategy, prone positioning, and management of the underlying cause.
Pathophysiology
ARDS involves widespread lung inflammation triggered by a direct or indirect injury to the alveolar-capillary membrane. This inflammation increases capillary permeability, allowing protein-rich fluid to flood the alveoli (pulmonary edema). The fluid-filled alveoli cannot participate in gas exchange, resulting in:
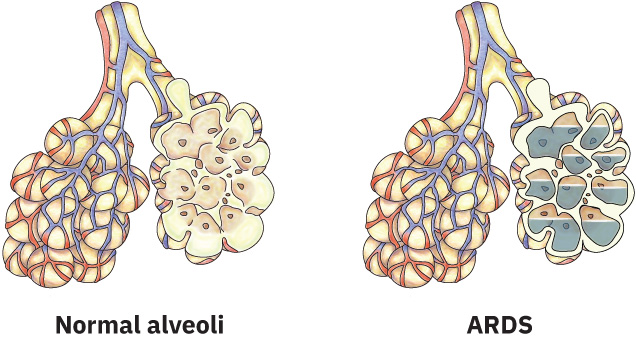 Illustration reference: OpenStax Medical-Surgical Nursing Ch.23.1.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.23.1.
- Severely decreased oxygenation (hypoxemia) refractory to supplemental oxygen
- Decreased lung compliance (stiff lungs requiring high ventilator pressures)
- V/Q mismatch and intrapulmonary shunting
Common Causes
| Direct (Pulmonary) | Indirect (Extrapulmonary) |
|---|---|
| pneumonia (Pneumonia) (including COVID-19) | sepsis (Sepsis) |
| Gastric aspiration | Burn injury |
| Near-drowning | Drug overdose |
| Trauma/chest injury | Multiple blood transfusions |
| Fatty embolism | Cardiopulmonary bypass |
Relationship to Shock and Sepsis
In the progressive stage of shock, substantial capillary permeability causes fluid to shift from capillaries into alveolar spaces, producing pulmonary edema, bronchoconstriction, decreased lung capacity, tachypnea, increased work of breathing, respiratory acidosis, and progression to ARDS.
Nursing Assessment
NCLEX Focus
The defining characteristic of ARDS on NCLEX is refractory hypoxemia — SpO₂ and PaO₂ that fail to improve despite high-flow supplemental oxygen. Any mechanically ventilated patient who develops worsening oxygenation with bilateral infiltrates should be evaluated for ARDS.
Diagnostic criteria (Berlin Definition):
- Acute onset within 1 week of a known clinical insult or new/worsening respiratory symptoms
- Bilateral lung infiltrates on chest X-ray of noncardiac origin (bilateral ground-glass opacities)
- PaO₂/FiO₂ ratio <300 mmHg despite PEEP ≥5 cmH₂O
Clinical assessment findings:
- Dyspnea and tachypnea progressing to respiratory alkalosis, then metabolic acidosis
- Decreased level of consciousness from cerebral hypoxia
- Restlessness, irritability, agitation
- Fine crackles throughout the lung fields
- SpO₂ that fails to rise despite high FiO₂ administration
- Decreasing PaO₂ on ABG despite supplemental oxygen
Nursing Interventions
Oxygenation support:
- Anticipate and prepare for endotracheal intubation and mechanical ventilation — the cornerstone of ARDS management.
- Maintain lung-protective ventilation strategy: low tidal volume (6 mL/kg ideal body weight), adequate PEEP to prevent alveolar collapse, limiting plateau pressure to ≤30 cmH₂O.
- Prone positioning: Repositioning the patient prone (face-down) for 12–16 hours improves V/Q matching and oxygenation by redistributing perfusion to less-damaged lung regions; requires a team-based approach to prevent pressure injuries, ETT dislodgement, and line complications.
Pharmacological management:
- Corticosteroids may be used to reduce inflammation in selected cases.
- Neuromuscular blocking agents may be used in the first 48 hours to reduce ventilator dyssynchrony and oxygen consumption.
- Sedation and analgesia are required for endotracheal intubation tolerance and to reduce work of breathing.
Supportive care:
- Maintain conservative fluid management to prevent worsening pulmonary edema.
- Monitor arterial blood gases (ABGs) frequently to guide ventilator adjustments.
- Implement VAP (ventilator-associated pneumonia) prevention bundle: head-of-bed elevation 30–45°, oral care, daily sedation vacation and spontaneous breathing trials.
- Monitor for and prevent complications: barotrauma (pneumothorax from high ventilator pressures), ICU-acquired weakness, and stress ulcers.
Refractory Hypoxemia
A patient whose SpO₂ or PaO₂ continues to decline despite escalating oxygen delivery is experiencing refractory hypoxemia — a critical sign that alveolar gas exchange is failing. Escalate to the provider immediately and prepare for intubation or ICU transfer. Do not delay action waiting for a single “perfect” reading.
Related Concepts
- respiratory-system — Normal alveolar gas exchange mechanisms disrupted in ARDS.
- respiratory-failure — ARDS as the most severe form of acute respiratory failure.
- evidence-based-respiratory-care — Lung-protective ventilation and VAP bundle as evidence-based practices.
- sepsis — Sepsis as the most common indirect cause of ARDS.
- bronchial-hygiene-techniques — Airway clearance support in mechanically ventilated patients.
- prioritizing-early-deterioration-cues-in-fluid-electrolyte-care — Early recognition of clinical deterioration patterns.
Self-Check
- What is the diagnostic criterion for ARDS regarding oxygenation, and why does refractory hypoxemia distinguish ARDS from less severe respiratory failure?
- A nurse is caring for a patient with ARDS who is receiving 100% FiO₂ via mechanical ventilator. The SpO₂ remains 84%. What position change intervention may be ordered, and what nursing considerations does it require?
- List two direct and two indirect causes of ARDS.