Spinal Cord Injury
Key Points
- Spinal cord injury causes temporary or permanent loss of sensory, motor, and autonomic function below injury level.
- Major causes include motor vehicle accidents and severe falls; higher lesions produce greater disability.
- High cervical injury can cause tetraplegia and life-threatening respiratory failure.
- SCI is classified as complete or incomplete based on preserved communication below the lesion.
- Long-term outcomes depend on early stabilization and aggressive complication prevention.
Pathophysiology
SCI results from direct cord trauma or secondary damage from surrounding vertebral injury, bleeding, and swelling. Neurologic deficits may appear immediately or progress as edema and hemorrhage worsen tissue injury.
Lesion height strongly predicts severity: higher lesions affect a larger body distribution. Cervical-level injury can impair diaphragmatic function and breathing. Nontraumatic causes such as malignant spinal involvement can also produce cord compression and permanent deficits when decompression is delayed.
Dermatomal mapping is clinically important because each spinal nerve serves a specific skin region; segment-level injury can therefore produce patterned sensory deficits across most of the body below the face.
Classification
- By neurologic completeness:
- Incomplete injury: Residual sensory or motor communication below lesion.
- Complete injury: No preserved communication below lesion.
- By level effects:
- High-level injury: Greater risk of tetraplegia and respiratory compromise.
- Lower-level injury: More likely paraplegia pattern.
- By cord syndrome pattern (incomplete injury subsets):
- Brown-Sequard syndrome: Hemicord lesion pattern with ipsilateral motor weakness and proprioceptive/light-touch loss plus contralateral pain-temperature loss.
- Central cord syndrome: Often cervical hyperextension injury pattern with disproportionate upper-extremity motor/sensory deficits and possible bladder dysfunction.
- Anterior cord syndrome: Often hyperflexion/fracture or acute disc-herniation pattern with motor and pain-temperature loss below lesion and relative preservation of light touch/vibration/position sense.
- Posterior cord syndrome: Posterior-column pathway injury (for example compression/vascular or demyelinating context) with proprioceptive-vibration loss, sensory ataxia, and impaired coordinated movement.
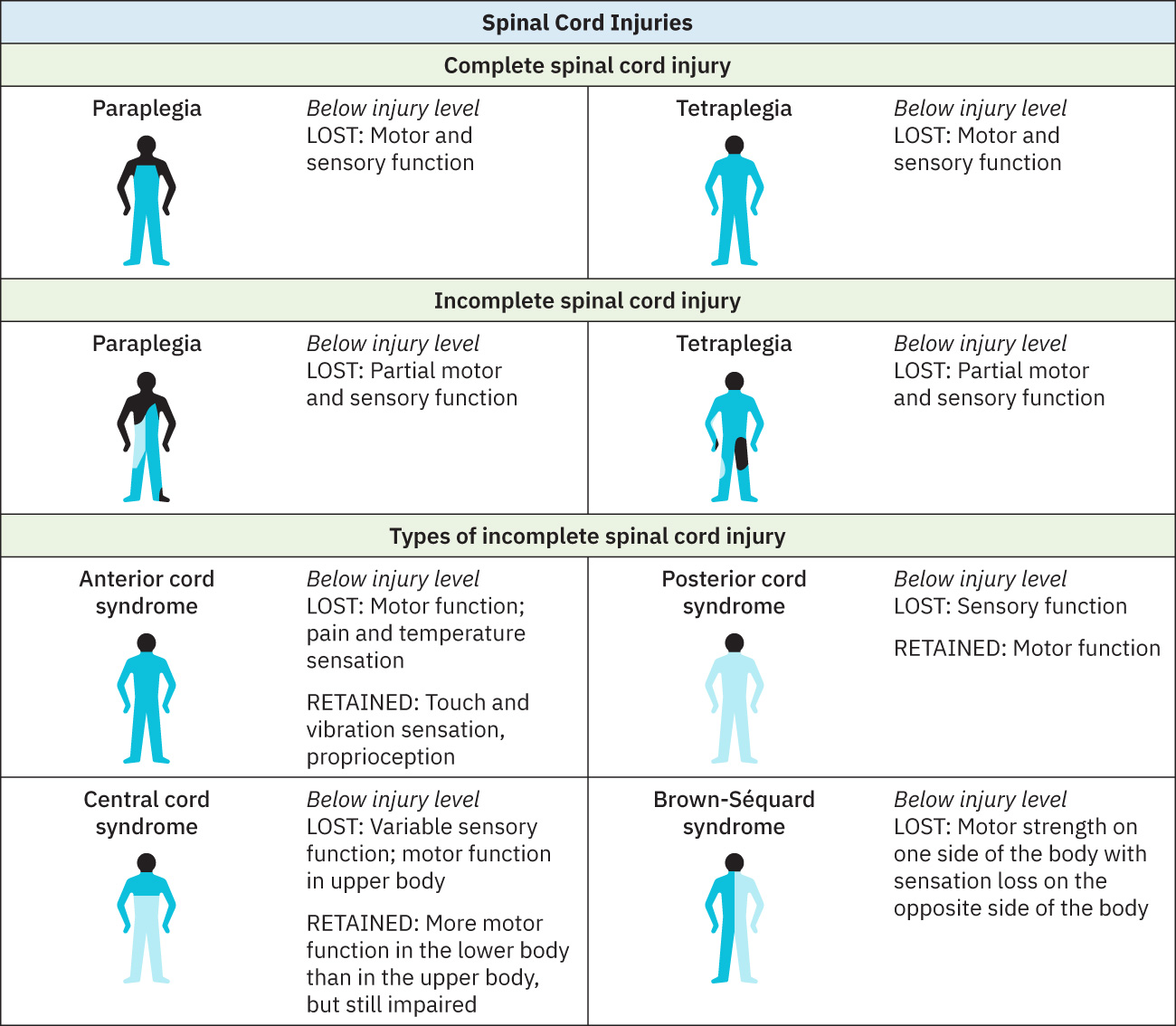 Illustration reference: OpenStax Clinical Nursing Skills Ch.26.3.
Illustration reference: OpenStax Clinical Nursing Skills Ch.26.3.
Nursing Assessment
NCLEX Focus
In acute SCI, prioritize airway/breathing, circulation, and progressive neurologic deficits.
- Assess mechanism and risk factors (high-impact trauma, falls, alcohol use, lack of protective gear).
- Assess distribution and progression of sensory/motor loss.
- Assess respiratory compromise risk, especially with cervical-level injury.
- Assess hemodynamic instability and shock patterns early after injury.
- Assess for evolving complications: dysautonomia, DVT risk, pressure injury, bowel/bladder dysfunction, and mood changes.
- Assess for paralysis-pattern sequelae including involuntary spasm, hyperreflexia, sexual dysfunction, and changes in bowel/bladder control.
- Do not assume absent pain sensation in paralyzed limbs; motor loss can coexist with preserved sensory pathways.
Diagnostic and Monitoring Data
- MRI: cord/soft-tissue and ligament injury, compression, inflammation, bleeding context.
- CT: bone fracture, bleeding, and spinal-canal narrowing detection.
- X-ray: vertebral alignment and fracture screening.
Nursing Interventions
- Support airway and ventilation needs; high cervical injuries may require temporary or permanent ventilatory support.
- Support perioperative care in clients requiring decompression or stabilization surgery.
- Assist with ordered traction and immobilization pathways to maintain spinal alignment.
- Implement aspiration precautions and pneumonia prevention.
- Prevent circulatory complications with ordered anticoagulation context and compression strategies.
- Prevent pressure injury with frequent repositioning (commonly every 1-2 hours in immobile clients).
- Implement bowel/bladder management plans, including catheter and bowel-program support as ordered.
- Monitor and treat spasticity, neurogenic pain, and functional decline with interdisciplinary input.
- During positioning and procedures, use pain-safety communication and analgesia planning even when movement is absent.
- Place suspected autonomic dysreflexia patients in upright/sitting position while trigger-focused management is initiated.
- Coordinate comprehensive rehabilitation for functional recovery, psychosocial adaptation, and quality-of-life optimization.
Multi-System Deterioration Risk
Respiratory, circulatory, skin, and autonomic complications can escalate rapidly without proactive prevention bundles.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Anticoagulation prophylaxis (context) | Protocol-driven | Reduces venous thromboembolism risk in severe immobility states. |
| Anti-inflammatory and edema-control contexts | NSAID and corticosteroid pathways by indication | May reduce pain/swelling burden in selected care pathways. |
| Spasm-control contexts | tizanidine, diazepam | Can reduce painful spasm burden; monitor sedation and respiratory safety. |
| Mood-pain modulators | SNRI contexts | May support concurrent pain and depressive symptom burden in selected chronic trajectories. |
| Bowel regimen agents (context) | Laxative protocols | Supports neurogenic bowel programs and complication prevention. |
| Pain-management regimens (context) | Multimodal | Needed for neurogenic and musculoskeletal pain burden. |
Clinical Judgment Application
Clinical Scenario
A patient with cervical SCI develops weak cough, rising secretions, and new blood-pressure instability.
- Recognize Cues: Respiratory deterioration and autonomic instability in high-risk lesion pattern.
- Analyze Cues: Multi-system SCI complications are emerging simultaneously.
- Prioritize Hypotheses: Airway/ventilation and hemodynamic stability are immediate priorities.
- Generate Solutions: Escalate respiratory support, strengthen complication-prevention bundle, and reassess for autonomic triggers.
- Take Action: Implement urgent respiratory-circulatory interventions and interdisciplinary review.
- Evaluate Outcomes: Oxygenation and perfusion stabilize while secondary complications are contained.
Related Concepts
- autonomic-dysreflexia - Life-threatening autonomic emergency in higher-level SCI.
- pressure-injury-staging-and-risk-assessment - Repositioning and skin surveillance are essential in paralysis.
- nursing-care-priorities-for-neuromuscular-impairment - Shared respiratory and mobility-risk framework.
- collaborative-and-environmental-neuromuscular-care - Rehabilitation and caregiver-support coordination.
Self-Check
- How do complete and incomplete SCI patterns differ in functional prognosis?
- Why are cervical SCI lesions especially dangerous for respiratory status?
- Which prevention bundle elements most reduce long-term SCI morbidity?