Transmission-Based Precautions
Key Points
- Transmission-based precautions are added when pathogen risk exceeds baseline control with standard-precautions alone.
- Categories are contact, droplet, and airborne precautions.
- PPE selection and workflow are determined by transmission route and expected exposure.
- Some diseases can require more than one transmission-based category when a single route control is insufficient.
- Single-room placement, dedicated equipment, and clear door signage improve isolation reliability.
- Signage and pre-entry nursing communication prevent wrong-PPE entry errors.
- Transport should be limited to essential needs and coordinated with receiving teams.
- Isolation workflows should include psychosocial support actions to reduce loneliness and perceived abandonment.
- High-consequence viral outbreaks require strict screening, immediate isolation, and disciplined PPE adherence to protect staff and families.
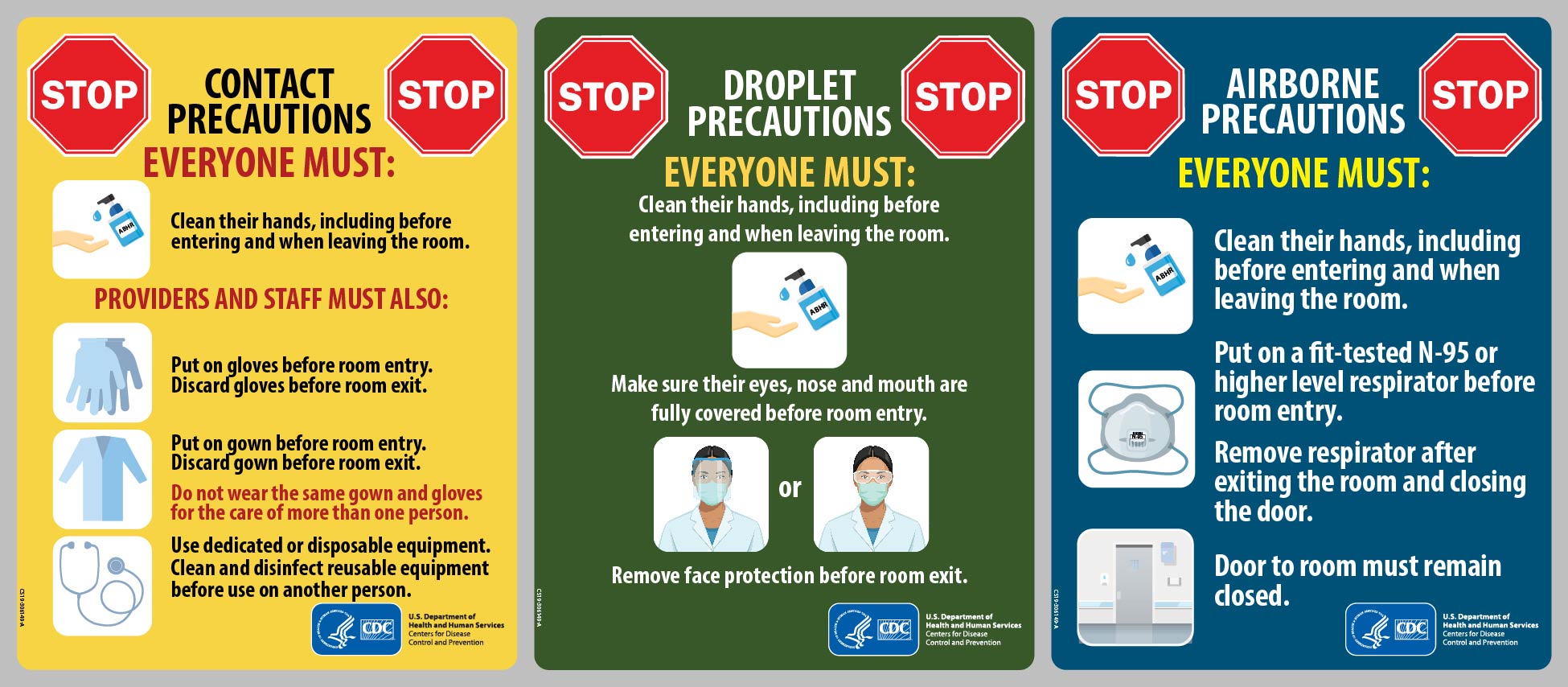 Illustration reference: OpenStax Clinical Nursing Skills Ch.6.
Illustration reference: OpenStax Clinical Nursing Skills Ch.6.
Pathophysiology
Transmission Based Precautions are route-specific controls designed to block the pathogen at its dominant mode-of-transmission. They are layered on top of standard-precautions when infection is known or suspected to spread easily in healthcare settings.
High-risk organisms and conditions requiring additional controls include MRSA, VRE, C. difficile, RSV, measles, tuberculosis, and COVID-related risks. The precaution category determines barriers and room practices needed to reduce spread to staff and other patients.
These measures are operational controls, not diagnosis labels. Correct use depends on understanding source site, task risk, and exposure pathway during specific care actions.
Classification
- Contact precautions: Gloves and gown; dedicated equipment; prioritize room disinfection; limit transport.
- Enhanced barrier precautions: Gloves and gown during high-contact resident-care activities for residents colonized/infected with MDROs or at increased MDRO-acquisition risk.
- Contact organism examples: MRSA, VRE, ESBL, C. difficile, carbapenemase-producing organisms (CPO), scabies, and selected diarrheal syndromes.
- Droplet precautions: Mask plus eye protection (goggles or face shield) for pathogens spread by large respiratory droplets; droplets typically travel up to about 2 meters (about 6 feet); patient wears a surgical mask for essential transport.
- Droplet condition examples: Influenza, mumps, and undifferentiated respiratory/GI symptom presentations (for example unconfirmed cough or vomiting of unknown cause) pending final diagnosis.
- Airborne precautions: Fit-tested N95 respirator with airborne infection isolation room (negative pressure), closed door, and restricted susceptible-person entry; if no negative-pressure room is available, use private-room isolation with patient masking and urgent escalation.
- Airborne organism examples: Tuberculosis, measles, varicella, disseminated zoster, and SARS-spectrum risk conditions.
- High-consequence outbreak workflow: For severe viral hemorrhagic or uncertain high-risk outbreaks, follow facility/public-health escalation protocols with strict barrier controls, hand hygiene, and suspect-case isolation.
Nursing Assessment
NCLEX Focus
Questions commonly ask which precaution category matches the pathogen route and the planned task.
- Review the care plan and current isolation status before room entry.
- Determine likely source and route of transmission for the suspected or confirmed pathogen.
- Assess the planned task for added splash or aerosol risk that changes PPE needs.
- Confirm required PPE is available and correctly donned before patient contact.
- Verify door signage and clarify uncertainties with the nurse prior to entry.
- Use nursing care-plan details (not public door text) to confirm pathogen source and required PPE.
Nursing Interventions
- Continue standard-precautions for all care, then add route-specific PPE.
- Use contact, droplet, or airborne protocol according to pathogen transmission route.
- For high-consequence outbreak alerts, front-load screening and isolate suspected cases immediately while awaiting definitive diagnosis.
- Keep transmission-precaution signage and PPE supply cart in place near room entry.
- Apply barriers during transport and limit movement to essential diagnostics or therapy.
- For airborne transport, ensure patient masking per policy (commonly respirator-level masking when available).
- Notify receiving personnel before transfer so precautions are ready on arrival.
- Maintain clear patient communication despite PPE and reduced contact time.
- Provide supportive explanation and frequent check-ins to reduce isolation-associated anxiety, depression, stigma, and perceived abandonment.
- Support practical family-contact options (for example phone/video access and charging support) to reduce isolation stress.
- Document and report breaches in isolation process immediately.
Airborne Suspected in Long-Term Care
Suspected airborne illness requires urgent escalation and transfer to settings with specialized air-handling capability.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Not specified in source | None provided in this section | Route-based isolation controls are the primary nursing intervention in this topic |
Clinical Judgment Application
Clinical Scenario
A resident with wound drainage is on contact precautions, then develops cough and frequent sneezing. Staff are preparing for room entry and possible transfer.
- Recognize Cues: Existing contact risk plus new respiratory symptom pattern.
- Analyze Cues: Transmission route may have changed, requiring upgraded barrier strategy.
- Prioritize Hypotheses: Incorrect precaution category is the highest immediate safety risk.
- Generate Solutions: Reassess category with nurse, update PPE requirements, and prepare receiving-area notification.
- Take Action: Apply corrected precautions, reinforce entry controls, and coordinate essential transport only.
- Evaluate Outcomes: Appropriate PPE compliance, controlled transfer, and no secondary exposure events.
Related Concepts
- standard-precautions - Baseline layer that remains active under all isolation categories.
- mode-of-transmission - Determines whether contact, droplet, or airborne controls are required.
- personal-protective-equipment - PPE mix changes by category and task.
- enteric-precautions - Adds fecal-route controls to contact precautions.
- reverse-isolation-neutropenic-precautions - Protective workflow for clients with profound immune compromise.
- healthcare-associated-infections - Isolation failures can drive preventable spread.
Self-Check
- What is the difference between contact and droplet precaution workflows?
- Why can the same patient require different PPE for different tasks?
- What pre-transport action is required before moving an isolated patient?