Respiratory System
Key Points
- The respiratory system delivers oxygen, removes carbon dioxide, and supports acid-base balance.
- Gas exchange occurs at alveoli-capillary interfaces and depends on airway patency and effective ventilation.
- Inspiration and expiration sustain oxygen uptake and carbon-dioxide elimination across the capillary-alveolar membrane.
- Typical room-air oxygen saturation is about 95-100% in healthy adults.
- Upper-airway and lower-airway structures work together to warm, filter, and conduct air to alveoli.
- Oxygen has limited plasma solubility, so most oxygen transport occurs through hemoglobin binding as oxyhemoglobin.
- Ventilation is primarily driven by carbon dioxide changes detected by central and peripheral chemoreceptors.
- Respiration is an involuntary neurologically controlled vital function centered in the medulla and pons.
- Age-related respiratory decline increases susceptibility to acute infection and activity intolerance.
- In older adults, reduced cough effectiveness and lower respiratory-muscle reserve increase hypoxia and secretion-retention risk; pulmonary hygiene, incentive spirometry, and upright positioning are key preventive supports.
- Pediatric airway and gas-exchange anatomy (smaller airways, fewer alveoli, weaker respiratory musculature) increases obstruction and fatigue risk during illness.
- Alveolar growth and maturation continue through childhood (approximately to age 8), so early-life insults can create persistent lung-function deficits.
Pathophysiology
Respiration maintains cellular metabolism by transporting oxygen into blood and eliminating carbon dioxide. Airway structures and respiratory muscles move air to alveoli, where capillary exchange links pulmonary function with cardiovascular transport.
Effective oxygen delivery also depends on adequate cardiac output/perfusion and sufficient hemoglobin carrying capacity; cardiovascular and hematologic compromise can worsen oxygenation even when airway mechanics are preserved.
With aging, chest muscle strength declines and bronchioles lose elasticity, increasing small-airway collapse risk and reducing ventilation efficiency. This decreases reserve during illness and increases risk of dyspnea, fatigue, and oxygenation instability.
The upper respiratory tract includes the nose, nasal cavity, sinuses, pharynx, and larynx. The lower respiratory tract includes the trachea, bronchi, bronchioles, alveoli, and lungs with pleural membranes. Coordinated function of these structures supports filtration, humidification, ventilation, gas diffusion, and pulmonary perfusion. The thoracic cavity includes pleural spaces surrounding the lungs and the pericardial space surrounding the heart. Within upper-airway structure, the larynx links pharynx to trachea and is built around thyroid, cricoid, and epiglottic cartilages with paired arytenoid/corniculate/cuneiform support for phonation and airway control. The trachea extends from larynx toward bronchi and is reinforced by multiple C-shaped hyaline cartilage rings with a posterior fibroelastic membrane and trachealis muscle that preserve patency while allowing dynamic caliber change. At the carina, strong reflex sensitivity helps trigger cough when foreign material reaches the bifurcation. Primary bronchi enter lungs at the hilum alongside vascular, neural, and lymphatic structures, then branch to smaller bronchioles and terminal airways leading to alveoli. Some clinical teaching frameworks use a practical airway boundary in which upper-airway description extends through the trachea to the carina and lower-airway description begins below the carina. The lungs are paired, pyramid-like organs resting above the diaphragm. The right lung is typically wider/shorter with three lobes, while the left has two lobes and a cardiac notch to accommodate the heart; each lung has a superior apex and diaphragmatic base. Each lung is covered by visceral pleura and opposed by parietal pleura lining the thoracic wall/mediastinum/diaphragm. The pleural cavity between layers contains a thin lubricating film that reduces friction during breathing and helps maintain lung apposition to the chest wall.
Mucus and cilia together form the mucociliary escalator that clears inhaled particles and microbes from upper airways. Smoking-related ciliary injury can impair this clearance and increase lower-respiratory colonization and infection risk. Cold air can slow ciliary movement and contribute to transient mucus accumulation and rhinorrhea.
Bronchioles differ from larger airways because cartilage support is no longer present; smooth-muscle tone becomes a major regulator of airflow. In alveoli, type II cells produce surfactant to reduce surface tension and limit alveolar collapse, while macrophages support local particle/pathogen clearance. Type I alveolar cells form most exchange surface area (commonly about 90%, around 70 m2), enabling efficient gas transfer.
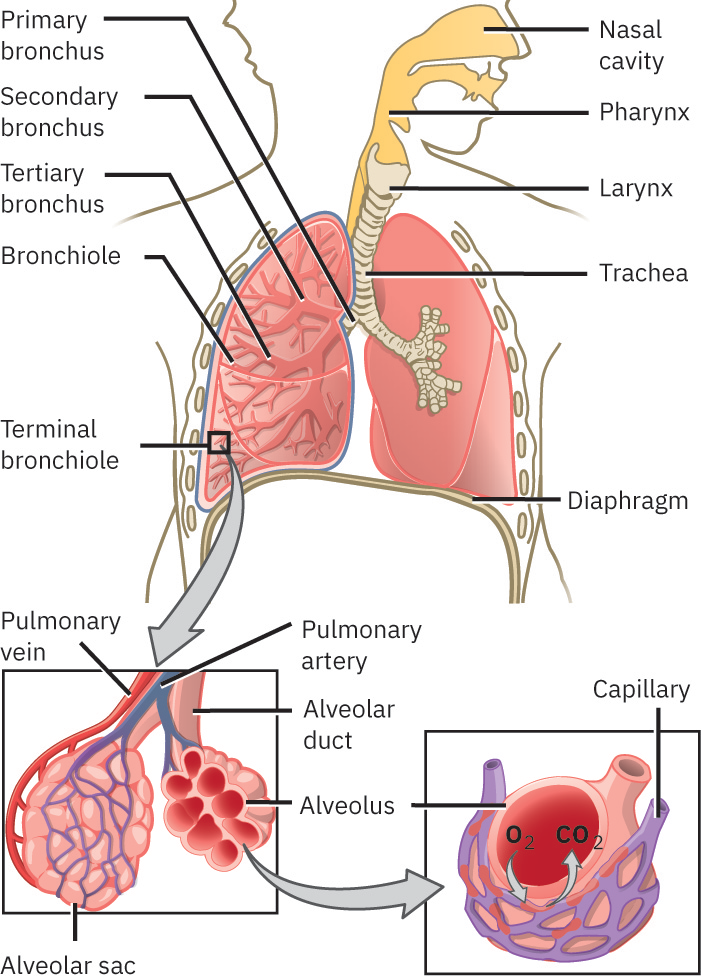 Illustration reference: OpenStax Clinical Nursing Skills Ch.18.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.18.1.
Pediatric respiratory anatomy introduces additional risk patterns: preterm/newborn surfactant insufficiency can increase alveolar-collapse risk; infants/young children have smaller caliber airways and relatively enlarged tonsillar tissue, increasing occlusion vulnerability during URI or secretion burden; infant tracheas are shorter and narrower with less margin for endotracheal-tube displacement; and respiratory muscles are less robust, increasing fatigue risk during sustained distress. Early-life exposure burden also matters: prematurity, IUGR context, and maternal/household smoke exposure can reduce long-term lung-function trajectory and increase later wheeze/asthma risk.
Chronic respiratory disorders vary in trajectory: some conditions (for example asthma) may remain stable over time, while others (for example COPD and pulmonary fibrosis) are commonly progressive and require tighter longitudinal surveillance.
Respiratory function also contributes to rapid acid-base compensation through carbon dioxide handling. Normal arterial pH is tightly regulated around 7.35-7.45; changes in respiratory rate/depth can alter CO2 elimination and shift pH toward normal. Gas diffusion occurs across an extremely thin respiratory membrane (about 0.5 micrometer), where O2 and CO2 movement is driven by concentration gradients.
Classification
- Ventilation components: Airway patency, respiratory-muscle effort, and lung expansion.
- Gas-exchange components: Alveolar-capillary diffusion and oxygen transport in hemoglobin.
- Upper-airway structures: Nares, nasal cavity, sinuses, pharynx (naso/oro/laryngopharynx), and larynx.
- Lower-airway structures: Trachea, bronchi/bronchioles, alveoli, and lungs with visceral/parietal pleura.
- Mechanical-lung-function components: Compliance (expandability) and elastic recoil (return toward baseline shape) support effective ventilation.
- Common chronic conditions: Asthma, COPD/emphysema, chronic rhinitis, sleep apnea, pulmonary fibrosis, cystic fibrosis, pneumonia, and lung-cancer contexts.
Nursing Assessment
NCLEX Focus
Priority questions center on identifying respiratory distress cues that require immediate nurse notification.
- Observe respiratory rate, effort, breath comfort, and ability to speak in full sentences.
- Treat one-word speech between breaths, marked accessory-muscle fatigue, and severe orthopnea as high-acuity deterioration cues.
- Use a 0-10 dyspnea rating to trend symptom severity over time and after interventions.
- Distinguish normal respiratory-rate ranges (adult 12-20/min) from tachypnea, bradypnea, and apnea patterns.
- Use age-adjusted pediatric respiratory-rate references: under 1 year about 30-60/min, around 10 years about 18-30/min, and adolescence about 12-18/min.
- In pediatric clients with recurrent wheeze or reduced exercise tolerance, assess developmental exposure history (prematurity/IUGR, maternal smoking, secondhand smoke, and recurrent RTI burden).
- In suspected sleep-disordered breathing, assess upper-airway risk pattern (obesity, neck circumference, supine sleep pattern, smoking, alcohol/sedative use) and escalate screening referral when indicated.
- Identify cyanosis, disorientation, dizziness, chest discomfort, or sudden fatigue escalation.
- Track cough pattern and sputum amount/color changes, especially blood-tinged or yellow-green-brown purulent sputum.
- Recognize that anxiety and dyspnea can amplify each other; rely on objective respiratory trends to guide escalation urgency.
- Use pulse oximetry trends as a noninvasive oxygenation indicator and escalate persistent saturation decline.
- Use ABG results when available to correlate ventilation, oxygenation, and acid-base status in respiratory compromise.
- Assess breath-sound abnormalities (rhonchi, crackles/rales, wheeze, stridor, pleural rub) and trend changes.
- In pediatric illness, treat rapid escalation of work of breathing as high risk when small-airway obstruction, tonsillar/pharyngeal crowding, laryngospasm tendency, or respiratory-muscle fatigue is suspected.
- Report blocked-airway signs and acute breathing changes immediately.
Nursing Interventions
- Position for breathing comfort and segment ADLs to reduce oxygen demand.
- Encourage hydration (if appropriate) to thin secretions and improve clearance.
- Promote smoking cessation and trigger avoidance for chronic airway disease.
- Reinforce respiratory health-promotion measures: annual influenza vaccination, indicated pneumococcal vaccination, and activity progression as tolerated.
- Reinforce prescribed oxygen use and activity pacing.
- Escalate signs of upper-airway obstruction and prepare emergent airway support when indicated.
- Escalate suspected severe V/Q mismatch cues (for example pulmonary edema or pulmonary embolism patterns).
- For sleep-apnea concern, support structured screening workflow (for example STOP-BANG) and reinforce risk-factor education.
- In older adults, maintain heightened surveillance during influenza, pneumonia, and COVID-19 illness windows because age-related reserve is reduced.
- In older adults and postoperative/bedrest contexts, reinforce turn-cough-deep-breathe routines, incentive spirometry, frequent oral hygiene, and upright positioning to reduce secretion burden and ventilation-perfusion mismatch.
Life-Threatening Airway/Oxygenation Risk
Any sudden breathing difficulty, cyanosis, or airway obstruction signs require immediate escalation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| bronchodilators | Asthma/COPD management context | Monitor symptom relief and report persistent distress after therapy use. |
| antibiotics | Bacterial pneumonia (pneumonia) context | Support adherence and monitor for fever, worsening cough, or confusion. |
Clinical Judgment Application
Clinical Scenario
An older resident with COPD becomes increasingly short of breath, dizzy, and mildly cyanotic during routine ambulation.
- Recognize Cues: Escalating dyspnea, activity intolerance, and oxygenation warning signs.
- Analyze Cues: Respiratory reserve is insufficient for current exertion and may worsen quickly.
- Prioritize Hypotheses: Immediate priority is preventing hypoxemic deterioration.
- Generate Solutions: Stop activity, position for comfort, seek nurse support, and prepare ordered oxygen measures.
- Take Action: Escalate promptly with objective symptom/timing details.
- Evaluate Outcomes: Breathing stabilizes and safe activity plan is adjusted.
Ventilation Gas Exchange and Perfusion
- Ventilation mechanics: Inhalation occurs when the diaphragm contracts and intrathoracic pressure falls; exhalation occurs when the diaphragm relaxes and thoracic volume decreases.
- Breathing control: The medulla and pons regulate rate/depth, with carbon dioxide concentration as the primary physiologic driver. Pontine apneustic and pneumotaxic centers fine-tune tidal volume and respiratory rate; respiratory centers also respond to oxygen and pH trends.
- Brainstem motor groups: Medullary dorsal and ventral respiratory groups coordinate inspiratory and expiratory muscle activation.
- Pressure framework: Pulmonary ventilation depends on atmospheric, intra-alveolar (intrapulmonary), and intrapleural pressures.
- Pressure gradient rule: Air moves from higher pressure to lower pressure; normal inspiration occurs when intra-alveolar pressure falls below atmospheric pressure.
- Intrapleural baseline: Intrapleural pressure remains negative relative to atmospheric/intra-alveolar pressure (commonly around
-4 mm Hgacross the cycle). - Altitude impact: Reduced atmospheric pressure at higher altitude lowers driving gradients and can alter breathing workload/oxygenation.
- External respiration: Oxygen diffuses from alveoli to pulmonary capillaries while carbon dioxide diffuses into alveoli for exhalation.
- Partial-pressure gradient rule: Gas diffusion follows partial-pressure differences between alveoli and capillary blood.
- Oxygen transport forms: Most oxygen is carried bound to hemoglobin, with a smaller fraction dissolved directly in plasma.
- Oxyhemoglobin formation: Hemoglobin-oxygen binding forms oxyhemoglobin, which gives arterial blood its bright red color.
- Perfusion: Pulmonary arteries deliver deoxygenated blood to alveolar capillaries; pulmonary veins return oxygenated blood to the left heart.
- Perfusion determinants: Tissue oxygen delivery depends on circulation quality, circulating blood volume, cardiac pumping effectiveness, and blood pressure.
- Adequate-perfusion profile: Sufficient cardiac contractility and circulating volume with baseline mentation, normal pulses, and warm dry skin.
- Clinical mismatch: V/Q mismatch causes hypoxia when ventilation or perfusion is impaired (for example pulmonary edema or pulmonary embolism).
- Perfusion-deterioration cues: Tachycardia, hypotension, tachypnea, mentation change, cool clammy pallor, edema/crackles, and reduced oxygen saturation suggest inadequate tissue delivery.
- Oxygenation-limiting factors: Hypoventilation, restricted chest-wall or diaphragmatic expansion, airway narrowing (for example asthma or angioedema), reduced hemoglobin mass (for example anemia or hemorrhage), alveolar-capillary damage (for example COPD), and unventilated/alveolar-filling states (for example atelectasis, pneumonia, or pulmonary hemorrhage).
- RAAS linkage: Pulmonary capillary ACE contributes to conversion of angiotensin I to angiotensin II, linking respiratory and blood-pressure regulation physiology.
Hypoxia Versus Hypoxemia
- Hypoxia: Reduced tissue oxygenation.
- Hypoxemia: Reduced partial pressure of oxygen in arterial blood.
- Relationship: Hypoxemia and hypoxia may coexist, but they are not synonymous.
Related Concepts
- cardiovascular-system - Oxygen transport depends on integrated cardiopulmonary function.
- mouth-throat-nose-and-sinus-assessment-and-abnormalities - Upper-airway assessment informs respiratory risk stratification.
- thorax-and-lung-assessment-breath-sounds-and-respiratory-patterns - Bedside pattern and auscultation findings guide escalation.
- chronic-obstructive-pulmonary-disease - Major chronic cause of dyspnea and reduced exercise tolerance.
- pneumonia - Acute infectious process requiring early recognition and escalation.
- respiratory-viral-infections - Viral respiratory illness patterns and infection-control focused nursing care.
- tuberculosis - Contagious respiratory infection requiring prolonged therapy and airborne precautions.
- lung-cancer - Primary pulmonary malignancy requiring staged diagnosis and multimodal care.
- oxygen-therapy - Common supportive intervention for hypoxemia management.
- incentive-spirometry-and-pulmonary-expansion - Deep-breathing education strategy that supports alveolar recruitment and atelectasis prevention.
- advanced-airways-and-intubation - Immediate escalation pathway in acute obstruction or severe distress.
Self-Check
- Which respiratory findings indicate urgent escalation versus routine monitoring?
- How do age-related airway changes increase risk during respiratory infections?
- Which nonpharmacologic interventions best reduce dyspnea during ADLs?