Five vital signs: Temperature (T), Pulse (P), Respiratory Rate (RR), Blood Pressure (BP), SpO2 — pain is often called the “fifth vital sign” in clinical practice
Delegation: Vital signs may be delegated to UAP for stable patients per state NPA and agency policy — nurse remains accountable for interpreting results and following up on deviations
Obtain vital signs at admission, routine interval, and any condition-trigger event (for example suspected infection, fall, or relevant medication change).
Sequence is patient-condition dependent: many workflows place pulse oximetry first, but in sudden unresponsiveness a carotid pulse check/CPR decision is prioritized.
Ordered frequency is the minimum monitoring cadence; any change in condition warrants immediate reassessment.
Typical cadence varies by setting and acuity (for example acute care often every 4-8 hours, critical-care/postprocedure as frequently as every 15-60 minutes, outpatient at visit start, and long-term-care daily or as needed).
Normal adult pulse: 60–100 bpm; assess rate, rhythm, force (0–3+ scale), and bilateral equality
Apical pulse: Most accurate; required before administering cardiac medications
Pulse rate (palpated) can differ from heart rate (auscultated) when cardiac contraction force is weak.
If radial pulse site is inaccessible (for example cast, arterial line, amputation, or dressing), use apical auscultation and assess other perfusion sites as indicated.
Orthostatic hypotension: Drop of ≥20 mmHg systolic or ≥10 mmHg diastolic within 3 minutes of standing — significant fall risk, especially in older adults
Equipment
Thermometer (oral, tympanic, axillary, rectal, or temporal) with probe covers
Pulse oximeter with appropriate probe site
Stethoscope
Sphygmomanometer (blood pressure cuff) — appropriately sized for patient arm
Well-conditioned adolescents and athletes may have resting rates around 40-50 bpm with adequate perfusion.
Respiratory Rate by Age
Age
Normal Range (breaths/min)
Infant
30–60
Toddler
20–30
Preschooler
20–25
School age
14–22
Adolescent
12–18
Adult
12–20
Blood Pressure (Adult Screening Categories)
Category
Systolic (mmHg)
Diastolic (mmHg)
Hypotension
<90
<60
Normal
90–119
60–80
Elevated
120–129
≤80
Stage I Hypertension
130–139
80–89
Stage II Hypertension
≥140
≥90
Oxygen Saturation (SpO2)
Typical healthy range: 94-100%
COPD patients: 88-92% may represent expected baseline
SpO2 is an estimate; severe anemia and poor peripheral perfusion can produce falsely low readings.
Pulse oximetry can be intermittent or continuous based on patient condition and clinical order.
Immediate Reporting Triggers (Adult)
Temperature greater than 38°C (100.4°F), noting older-adult baseline temperatures may be lower (about 36°C/96°F can be typical).
Pulse less than 60 bpm or greater than 100 bpm at rest.
Respiratory rate less than 12 or greater than 20 breaths/min.
Blood pressure outside normal range or with concerning symptoms.
Procedure Steps
Gather equipment — select thermometer route appropriate for patient age, level of consciousness, and condition; ensure BP cuff fits correctly (too small → falsely high reading; too large → falsely low reading)
Confirm timing/indication and prepare patient — verify ordered/routine schedule, monitoring parameters, trigger context (new symptoms, post-fall, medication-related reassessment), and relevant prior trends/history; screen for route/site restrictions (for example avoid BP in mastectomy/lymphedema-risk arm, avoid oral temperature with oral trauma, avoid compromised pulse sites); then perform hand hygiene, clean the stethoscope before patient contact, confirm two identifiers (patient states name/DOB while wristband is checked, plus second identifier per policy such as barcode scan/MAR match/LTC staff verification/photo match), explain procedure, and ensure patient has been resting; temperature: wait 15–25 minutes after hot/cold intake, smoking, or gum chewing before oral measurement; blood pressure: avoid caffeine/smoking/exertion for about 30 minutes when feasible, keep patient quiet, and allow at least 5 minutes seated rest
Obtain temperature — insert thermometer per route-specific technique; document route alongside temperature value (e.g., “37.0°C oral”)
Assess pulse — palpate radial pulse for 60 full seconds if irregular; assess rate, rhythm (regular/irregular), force (0 = absent, 1+ = weak/thready, 2+ = normal, 3+ = bounding), and bilateral equality. If radial site is inaccessible or too weak/rapid to interpret reliably, auscultate apical pulse for one full minute and consider brachial/femoral palpation to evaluate peripheral perfusion; for cardiac medications (for example digoxin): use apical method
Adjust pulse method by patient context — obtain pulse when resting/comfortable whenever feasible; if not feasible (for example pain, infant crying, acute stress), document circumstances and reassess as needed. In newborns and children under about 5 years, prioritize brachial or apical assessment when radial palpation is difficult.
Count respiratory rate — count for 60 seconds while appearing to assess pulse (to prevent patient from altering breathing); assess rhythm and depth/quality (no accessory muscle use, no nasal flaring); if chest movement is difficult to observe, auscultate one lung field with stethoscope for 60 seconds
Obtain SpO2 — apply probe to finger, toe, or earlobe; remove nail polish and account for artificial nails when finger probe is used; warm extremity if cold/vasoconstricted; if needed, use alternate site (for example earlobe or forehead/taped pediatric sensor); read value after stable waveform displayed; use continuous monitoring when ordered for unstable or high-risk patients
Measure blood pressure — wrap cuff snugly around upper arm (brachial artery); inflate 30 mmHg above point where radial pulse disappears; deflate at 2–3 mmHg/second; first Korotkoff sound = systolic; last Korotkoff sound = diastolic
Assess for orthostatic hypotension if indicated — measure BP and pulse supine (or seated baseline), then standing, then again at 3 minutes standing using the same arm and same equipment; orthostatic hypotension = SBP drop ≥20 mmHg or DBP drop ≥10 mmHg; pulse increase ≥30 bpm also significant. If symptoms persist without documented orthostatic change, repeat measurement because some patients show delayed decreases after more than 3 minutes standing.
Analyze and document results — immediately compare to patient’s baseline and age-specific normals; document with route (temperature), position (BP), room-air versus supplemental-oxygen context for SpO2, and clinical context; if monitor-derived values do not fit bedside findings, manually recheck and document discrepancy resolution
Report deviations — immediately notify provider or instructor of any out-of-range vital sign; when escalating change in status, report a complete current set for full clinical picture; follow agency policy for out-of-range follow-up actions; initiate emergency response for signs of deterioration (see tanners-clinical-judgment-model-in-nursing-practice)
Use condition-priority sequencing when unstable — if the patient acutely loses consciousness, check carotid pulse first to determine immediate CPR need before routine full-set sequencing.
Common Errors
Taking oral temperature <15 minutes after hot/cold intake → falsely elevated or decreased reading
BP cuff too small → falsely HIGH reading; cuff too large → falsely LOW reading
Palpating both carotid arteries simultaneously → risk of decreased cerebral blood flow; always assess one side at a time
Nail polish on SpO2 probe finger → falsely LOW SpO2 reading
Counting respiratory rate with patient aware → patient may voluntarily alter breathing pattern
Ignoring site contraindications (for example BP cuff on affected post-mastectomy arm) → preventable harm and invalid readings
Continuing to use suspected faulty equipment → repeated invalid data; remove from service, label do not use, and report for biomed check
Failing to disinfect stethoscope before/after assessment → avoidable cross-transmission risk
Related
oxygen-therapy — SpO2 targets and oxygen delivery decisions based on vital signs
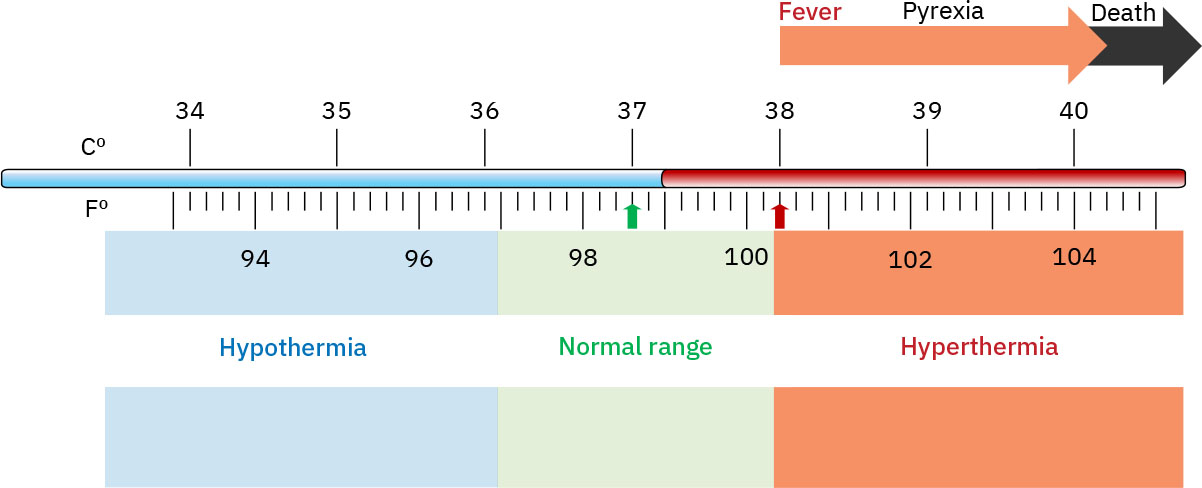 Illustration reference: OpenStax Fundamentals of Nursing Ch.7.2.
Illustration reference: OpenStax Fundamentals of Nursing Ch.7.2.