Aneurysm Assessment and Management
Key Points
- An aneurysm is dilation of a blood vessel from wall weakness and can progress to rupture or dissection.
- Major risk factors include hypertension, atherosclerosis, smoking, trauma, infection, and older age.
- Many aneurysms are initially asymptomatic and discovered incidentally on imaging.
- Worsening pain, hypotension, syncope, neurologic deficits, or signs of poor perfusion require urgent escalation.
- Management is based on aneurysm size, location, growth, symptoms, and hemodynamic stability.
- Chapter prevalence context includes AAA burden around 4-8% in U.S. populations, with rupture/dissection risk concentrated in unstable lesions.
- AAA surveillance/intervention uses size thresholds: annual imaging around 4.0-4.9 cm and elective endovascular repair commonly at greater than 5.5 cm.
Pathophysiology
Aneurysm forms when vascular wall integrity weakens and intraluminal pressure drives progressive dilation. Arterial aneurysms are common because arterial pressure places greater stress on compromised vessel walls. Key complications are rupture with life-threatening hemorrhage and dissection with an intimal tear that creates a false lumen.
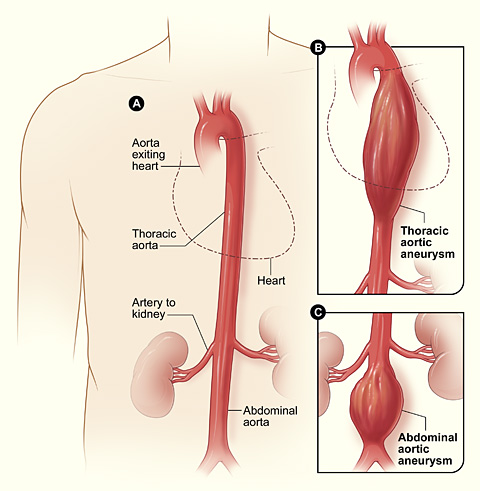 Illustration reference: OpenRN Health Alterations Ch.5.12.
Illustration reference: OpenRN Health Alterations Ch.5.12.
Progression risk increases when modifiable and nonmodifiable factors coexist, especially uncontrolled blood pressure and smoking exposure. Clinical deterioration may be sudden after a period of minimal or no symptoms. In AAA pathways, sclerotic aortic narrowing and ongoing high-pressure pulsatile stress can drive endothelial stretching, progressive outpouching, and eventual dissection/rupture if wall integrity fails.
Classification
- Stable or smaller aneurysm pattern: often asymptomatic and monitored by serial imaging.
- Enlarging or symptomatic pattern: pain and multisystem manifestations increase concern for instability.
- Rupture/dissection emergency pattern: abrupt severe symptoms and potential hemodynamic collapse.
- Ruptured AAA pattern: sudden severe abdominal/back pain with pulsatile abdominal findings, hypotension, tachycardia, and possible intra-abdominal hemorrhage.
Nursing Assessment
NCLEX Focus
Prioritize recognition of instability and rupture-risk cues over isolated chronic discomfort findings.
- Assess for pulsatile mass, bruit, new murmur over affected artery, hypotension, and syncope.
- Assess large-aneurysm systemic symptom clusters (for example diaphoresis, dizziness, fainting, tachycardia, nausea/vomiting, dyspnea, and sudden severe abdominal pain).
- Assess neurologic findings such as severe headache, visual disturbance, weakness, numbness, paralysis, or slurred speech.
- Assess respiratory and gastrointestinal cues including dyspnea, cough, abdominal tenderness, deep tearing abdominal pain, hematemesis, melena, distension, and palpable mass.
- Assess musculoskeletal and perfusion findings, including lumbar back pain, flank pain, cool or pale extremities, cyanosis, pallor, and diaphoresis.
- Assess symptom trend, risk factors, and emotional response, because anxiety often rises when rupture risk is discussed.
Diagnostic Testing Cues
- Anticipate ultrasound for initial screening and size/location trend review.
- For AAA pathways, ultrasound is common first-line detection and serial-size follow-up modality.
- Anticipate CTA for detailed cross-sectional vascular anatomy and complication evaluation.
- Abdominal/pelvic CT is commonly used when rupture-risk or complication detail is needed.
- Anticipate MRA as a noninvasive vascular imaging option.
- Anticipate angiography to define vascular compromise extent when procedural planning is needed, including combined CAD-plus-AAA workup contexts.
Nursing Interventions
- Escalate suspected rupture or dissection immediately.
- In unstable suspected rupture, maintain bed rest and activate rapid-response/emergency pathway immediately.
- Support watchful-waiting plans with blood pressure control, smoking cessation coaching, and follow-up imaging adherence.
- Administer prescribed antihypertensive therapy and reinforce purpose, schedule, and side-effect reporting.
- Prepare and monitor perioperative care for EVAR, open repair, coiling, or clipping when indicated.
- For endovascular AAA repair education, reinforce that femoral-artery guidewire access is used to place an expandable stent graft that supports arterial-wall stability and preserves flow.
- After AAA repair, trend distal pulse quality/character and monitor access or incision sites (including limb-straight/flat restrictions when ordered for endovascular access healing).
- Provide clear teaching on worsening symptoms that require immediate provider contact or emergency care.
- Use therapeutic communication and psychosocial support to reduce fear and improve care-plan adherence.
Rupture and Dissection Emergency
Sudden severe pain with hypotension, syncope, acute neurologic change, or evidence of poor perfusion is an emergency requiring immediate rapid-response escalation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| beta blockers | class-based agents | Reduce blood pressure force on vessel walls and support progression-risk reduction. |
| ACE inhibitor therapy | class-based agents | Support long-term blood pressure control and vascular protection strategies. |
| antihypertensive therapy | multidrug regimens | Reinforce adherence and monitor for hypotension, dizziness, and trend response. |
| analgesic therapy | ordered pain-control use | Manage pain while preserving frequent reassessment for instability signs. |
Clinical Judgment Application
Clinical Scenario
A client with hypertension and smoking history reports sudden severe abdominal and back pain with dizziness and pallor.
- Recognize Cues: High-risk pain pattern and instability indicators are present.
- Analyze Cues: Findings are concerning for aneurysm rupture or dissection.
- Prioritize Hypotheses: Immediate threat is hemorrhagic and perfusion collapse.
- Generate Solutions: Activate emergency pathway and prepare diagnostics/intervention support.
- Take Action: Escalate rapidly with objective trend reporting and continuous monitoring.
- Evaluate Outcomes: Time-to-definitive vascular management is minimized.
Related Concepts
- hypertension-assessment-and-management - Blood pressure control is central to aneurysm progression-risk reduction.
- cardiovascular-and-peripheral-vascular-nursing-assessment - Focused vascular assessment supports rapid instability recognition.
- abdominal-organ-enlargement-and-vascular-red-flags - Abdominal vascular findings overlap with aneurysm emergency cues.
- peripheral-vascular-system-and-insufficiency-patterns - Vascular pathology patterns and diagnostic pathways are closely related.
- postoperative-pacu-priorities-and-complication-surveillance - Postprocedure surveillance is essential after aneurysm repair.
Self-Check
- Which symptom patterns should trigger immediate rupture/dissection escalation?
- How do ultrasound, CTA, MRA, and angiography differ in aneurysm evaluation workflow?
- Why are blood pressure control and smoking cessation emphasized in long-term management?