Antiemetics
Key Points
- Multiple drug classes treat nausea/vomiting by targeting different neurotransmitter receptors in the chemoreceptor trigger zone (CTZ) and vomiting center
- Ondansetron (Zofran): Serotonin antagonist — first-line for chemotherapy-induced nausea/vomiting (CINV) and postoperative nausea
- Prochlorperazine: Dopamine antagonist — effective but causes extrapyramidal symptoms (EPS) with prolonged use
- Metoclopramide: Prokinetic — speeds gastric emptying; risk of tardive dyskinesia with long-term use (Boxed Warning)
- Meclizine: Antihistamine — first-line for motion sickness and vertigo
- Scopolamine: Anticholinergic transdermal patch — motion sickness prevention; remove before MRI (metallic aluminized membrane)
- Promethazine carries a severe pediatric respiratory-depression warning and should not be used in children younger than 2 years.
Pathophysiology of Nausea and Vomiting
The chemoreceptor trigger zone (CTZ), located in the area postrema of the brain, receives input from multiple pathways and is not restricted by the blood-brain barrier — allowing it to detect toxins in the bloodstream (e.g., opioids, chemotherapy agents, anesthesia).
CTZ receives input from:
- GI tract (via cranial nerves IX and X) — distension, obstruction, inflammation
- Vestibular system — motion sickness, vertigo
- Cerebral cortex — odors, anxiety, pain
- Bloodstream — drugs, toxins, metabolic disturbances
The CTZ activates the vomiting center in the medulla → retro-peristaltic contractions + abdominal muscle contraction → emesis.
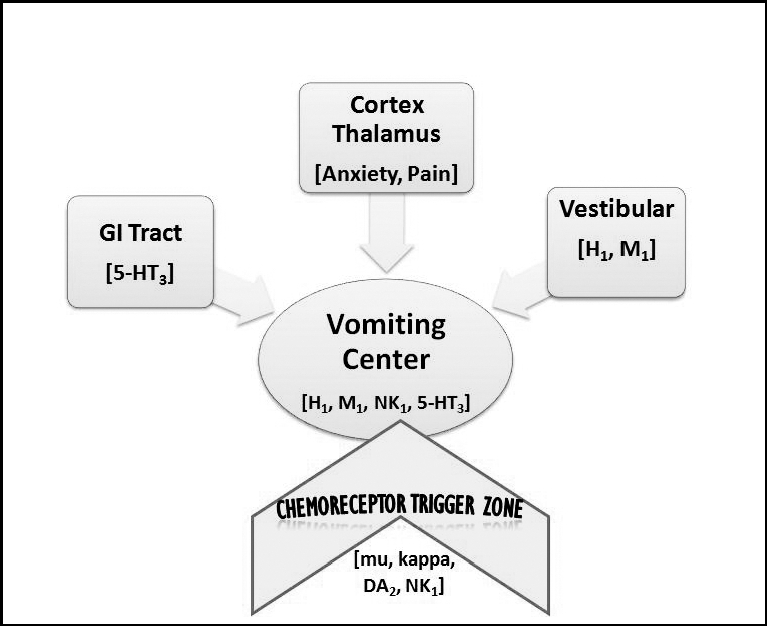 Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.5.
Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.5.
Escalation red flags: vomiting >24 hours, hematemesis, severe abdominal pain, severe headache/stiff neck, or worsening dehydration signs.
Drug Classes and Mechanisms
| Neurotransmitter | Drug Class | Prototype | Mechanism |
|---|---|---|---|
| Serotonin (5-HT3) | Serotonin antagonists | Ondansetron | Blocks 5-HT3 in GI tract, CTZ, and vomiting center |
| Dopamine (D2) | Dopamine antagonists | Prochlorperazine | Blocks dopamine in CTZ |
| Dopamine + ACh | Prokinetics | Metoclopramide | Blocks dopamine in CTZ + stimulates ACh in GI tract |
| Histamine (H1) | Antihistamines | Meclizine | Blocks H1 receptors → blocks ACh in vestibular system |
| Acetylcholine (M1) | Anticholinergics | Scopolamine | Blocks ACh receptors in vestibular system |
| Substance P (NK1) | Neurokinin antagonists | Aprepitant | Blocks NK1 receptors — used for CINV |
| Cannabinoid (CB1) | THC | Dronabinol | Activates CB1 receptor — inhibitory effect on CTZ |
Serotonin Antagonists (5-HT3 Antagonists)
Ondansetron (Zofran): Most widely used antiemetic in clinical practice.
Indications: Chemotherapy-induced nausea and vomiting (CINV), postoperative nausea and vomiting (PONV), radiation-induced nausea.
Advantages: Excellent safety profile; does not cause sedation or EPS; safe in pregnancy (used for hyperemesis gravidarum).
Routes: Oral, ODT (orally disintegrating tablet), IV, IM. Common pregnancy-context dosing reference: 4-8 mg every 8 hours as prescribed. IV timing profile: Onset often within about 15 minutes, peak around 30 minutes, and duration about 4-8 hours. IV administration safety: Give by slow IV push per protocol (commonly over about 2-5 minutes in adult practice) and reassess IV-site patency during/after administration to reduce infiltration or extravasation risk.
Contraindications/major interactions: Contraindicated with apomorphine; serotonin syndrome risk rises with concurrent serotonergic agents (e.g., SSRIs).
Adverse Effects: Headache, constipation, QTc prolongation with IV use (monitor ECG in at-risk patients), hypersensitivity reactions (fever/chills/rash/breathing difficulty).
Dopamine Antagonists
Prochlorperazine (Compazine): Blocks dopamine D2 receptors in the CTZ.
Indications: Severe nausea and vomiting, migraine-associated nausea.
Routes: PO, IM, PR, IV.
Contraindication (pediatrics): Avoid in children under 2 years old or under 20 lb.
Adverse Effects:
- Extrapyramidal Symptoms (EPS): Akathisia, dystonia, drug-induced parkinsonism — especially with prolonged use
- Sedation, orthostatic hypotension
- Tardive dyskinesia (long-term use)
- Photosensitivity and pink-to-reddish-brown urine can occur
Teaching: Avoid alcohol and other CNS depressants; use caution in extreme temperatures.
Phenothiazine Safety Alerts
- Promethazine: Severe respiratory depression and death can occur in children younger than 2 years (boxed warning).
- Chlorpromazine/Prochlorperazine: In older adults with dementia-related psychosis, antipsychotic exposure is associated with increased mortality risk.
- Phenothiazines can worsen orthostatic hypotension and sedation; apply fall-risk precautions and reassess hemodynamic tolerance.
Prokinetics — Metoclopramide (Reglan)
Mechanism: Blocks dopamine D2 receptors in the CTZ AND stimulates acetylcholine receptors in the GI tract → accelerates gastric emptying.
Indications: Diabetic gastroparesis, GERD, PONV, N/V when gastric emptying delay is a component.
Onset by route: IV 1-3 minutes, IM 10-15 minutes, PO 30-60 minutes; effects usually persist 1-2 hours.
Important contraindications:
- Do not use when increased GI motility is dangerous (GI hemorrhage, mechanical obstruction, perforation)
- Contraindicated in pheochromocytoma (risk of hypertensive crisis)
- Avoid in epilepsy or with other EPS-provoking medications when possible
Metoclopramide Boxed Warning — Tardive Dyskinesia
Tardive dyskinesia (irreversible involuntary movements) has been reported with metoclopramide. Risk increases with duration of use and cumulative dose. Avoid use >12 weeks unless clinical benefit outweighs risk.
Adverse Effects: EPS, drowsiness, fatigue, restlessness (akathisia), depression/suicidal ideation risk (especially with prolonged use), rare neuroleptic malignant syndrome.
Urgent teaching point: Report involuntary movements immediately (lip smacking, tongue thrusting, abnormal eye/limb movements).
Antihistamines
Meclizine (Antivert): Blocks H1 receptors, secondarily blocking acetylcholine in the vestibular system.
Indications: Motion sickness (first-line), vertigo associated with vestibular disorders.
Nursing considerations: Start about 1 hour before travel for motion-sickness prevention. Avoid use in glaucoma or enlarged prostate.
Adverse Effects: Drowsiness, dry mouth, blurred vision, constipation — classic anticholinergic effects.
Teaching: Avoid alcohol/sedatives; use caution with driving or machinery.
Hydroxyzine (Vistaril): First-generation H1 antagonist with antiemetic/anticholinergic effects used in anesthesia-associated, motion-related, and pregnancy-associated nausea pathways.
- Injectable hydroxyzine should be given by deep IM route into a large muscle (for example gluteal in adults; vastus lateralis in pediatric pathways).
- Monitor sedation burden and anticholinergic effects when co-administered with other CNS-active medications.
Dimenhydrinate: First-generation antihistamine option used in motion-related nausea and selected postoperative nausea pathways.
- Common adverse effects include drowsiness, dry mouth, and dizziness.
- Use fall-risk and sedation precautions when combined with other CNS depressants.
Pyridoxine-Doxylamine Combination (Pregnancy Nausea)
This combination is commonly used as first-line pharmacologic treatment when nonpharmacologic nausea measures are insufficient in pregnancy.
- Typical administration pattern: Often started as bedtime dosing, with additional daytime doses per prescription if symptoms persist.
- Mechanism pair: Pyridoxine (vitamin B6 support) plus doxylamine (H1-antihistamine/anticholinergic anti-nausea effect).
- Important caution: Avoid concurrent MAOI therapy due to interaction risk.
- Common side effects: Drowsiness, dry mouth/throat, dizziness.
Anticholinergics
Scopolamine (Transderm Scōp): Transdermal patch releasing ~1 mg over 3 days.
Application: Apply to hairless skin behind the ear (postauricular area). Only one patch at a time; do not cut the patch.
- For motion-sickness prevention, apply about 4 hours before travel when prescribed.
Indications: Prevention of motion sickness, postoperative nausea (associated with anesthesia and opioids).
MRI Contraindication
Scopolamine transdermal patches contain an aluminized membrane — remove before MRI to prevent skin burns at application site.
Adverse Effects: Dry mouth, blurred vision, drowsiness, confusion and memory impairment (especially in older adults), urinary retention.
Contraindication: Narrow-angle glaucoma.
Teaching: Use gloves for application/removal when feasible, fold patch adhesive-to-adhesive for disposal per policy, wash hands after handling, and avoid hazardous tasks (e.g., driving/operating machinery) until individual response is known.
Neurokinin Receptor Antagonists
Aprepitant: Commonly used with dexamethasone plus ondansetron for CINV/PONV prevention pathways.
Rolapitant: Oral NK1 antagonist option used before chemotherapy to help prevent acute and delayed CINV.
Major interaction points:
- Clinically significant CYP3A4 interactions (e.g., pimozide, diltiazem, rifampin)
- Can lower warfarin INR effect; increase INR monitoring when co-administered
- Can reduce efficacy of oral contraceptives; use backup birth control
Common adverse effects: Fatigue, dizziness, constipation, decreased appetite.
THC (Dronabinol/Medical Marijuana)
Use case: Refractory chemotherapy-associated nausea/vomiting (or cancer/AIDS-related nausea and appetite loss) when other antiemetic options are insufficient.
Nursing considerations:
- Psychoactive and dose-related CNS effects (elation, altered perception, impaired coordination)
- In older adults, start low and titrate cautiously due to higher sensitivity and postural hypotension risk
- Habit-forming potential; counsel on safety and secure storage
- Use caution in pregnancy and breastfeeding due to potential fetal/neurodevelopmental risk.
Teaching: Do not drive/operate machinery while affected.
For chemotherapy-associated nausea, ondansetron-centered pathways can reduce CNS-depression and infusion-site irritation burden compared with older phenothiazine antiemetic strategies.
Nursing Assessment
Before Administration:
- Identify the cause of nausea/vomiting — target treatment to the cause
- Assess hydration status: skin turgor, mucous membranes, urine output and color, blood pressure, heart rate
- Lab values if ordered: Hgb, Hct, serum sodium (dehydration markers)
- Document frequency, amount, and character of emesis
During/After Administration:
- Monitor for improvement in nausea and frequency of vomiting
- Assess for adverse effects (EPS with prochlorperazine/metoclopramide)
- Monitor continued fluid balance
- Report persistent vomiting >24 hours, hematemesis, severe abdominal pain, or severe headache with stiff neck
Patient Education — Nonpharmacological Measures:
- Drink small sips of clear liquids frequently — avoid large amounts
- Eat bland foods; avoid spicy, fatty, or salty foods
- Eat smaller, more frequent meals
- Avoid strong smells that trigger nausea
- Prefer room-temperature meals/fluids and avoid high-bulk meals when nausea is active
- Use adjunct relaxation and music-therapy strategies to reduce symptom intensity
- Consider peppermint-oil aromatherapy as an adjunct when compatible with facility policy and patient preference
- For morning sickness: eat plain crackers before rising
- Adjunct options sometimes used in pregnancy-related nausea include ginger (up to 2 g/day in divided doses) and pyridoxine 10-25 mg every 8 hours when clinically appropriate
Related Concepts
- diarrhea-assessment-and-management — GI distress management
- constipation — Opioid-induced constipation
- fluid-volume-deficit-hypovolemia-and-dehydration — Dehydration from persistent vomiting
- pain-management — Opioid-induced nausea management
- antidepressants — Ondansetron used with serotonergic drugs — serotonin syndrome risk
- postoperative-pacu-priorities-and-complication-surveillance — PONV as common postoperative complication
Self-Check
- A patient undergoing chemotherapy develops severe nausea. Which antiemetic class (and specific drug) is first-line for chemotherapy-induced nausea, and what is its mechanism?
- A patient who has been taking metoclopramide for 6 months develops repetitive lip-smacking movements and tongue thrusting. What adverse effect has occurred, and what is its significance?
- A patient with a scopolamine patch is scheduled for an MRI. What action must the nurse take before the scan, and why?