Gastroesophageal Reflux Disease GERD
Key Points
- GERD is chronic backflow of stomach contents into the esophagus.
- Disease burden is common in adults and can progress from symptom-only reflux to mucosal injury.
- Core risk factors include lower-esophageal-sphincter dysfunction, hiatal hernia, delayed gastric emptying, obesity, tobacco/alcohol use, pregnancy, and selected medications.
- Nursing priorities are symptom control, risk-factor modification, and prevention of erosive or premalignant esophageal complications.
Pathophysiology
GERD occurs when refluxed gastric contents repeatedly contact esophageal mucosa because normal antireflux barriers are weakened. Lower-esophageal-sphincter tone abnormalities, pressure-related anatomy changes (for example hiatal hernia), delayed gastric emptying, and impaired esophageal clearance mechanisms increase reflux exposure.
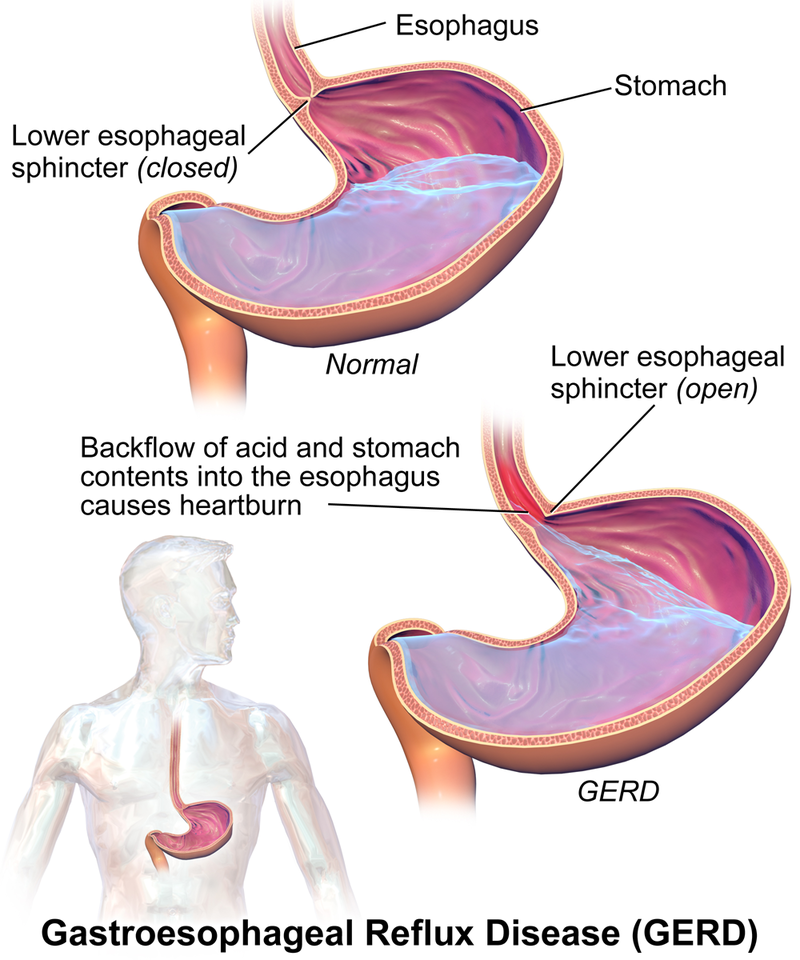 Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.3.
Illustration reference: OpenRN Nursing Pharmacology 2e Ch.7.3.
Normally refluxed acid is cleared by esophageal peristalsis and buffered in part by salivary bicarbonate. When these defenses are impaired, mucosal injury accumulates. Persistent reflux can evolve from nonerosive symptoms to visible esophageal injury and, in selected clients, metaplastic change risk.
Chronic reflux injury can drive replacement of normal squamous epithelium with intestinal-type cells (Barrett pattern), increasing esophageal adenocarcinoma risk over time.
Classification
- Nonerosive reflux disease: Reflux symptoms without visible esophageal erosion.
- Erosive esophagitis: Reflux with erosions or ulceration of esophageal mucosa.
- Barrett esophagus spectrum: Intestinal metaplasia risk state associated with chronic reflux exposure.
Nursing Assessment
NCLEX Focus
Distinguish uncomplicated reflux symptoms from cues of progressive mucosal injury.
- Assess typical symptom pattern, including postprandial or recumbent retrosternal burning (heartburn) and acid regurgitation.
- Screen associated symptoms such as dysphagia/odynophagia, nausea, epigastric pain, and frequent belching.
- Recognize atypical presentations, including chronic cough, hoarseness/laryngitis, chest pain, new-onset asthma pattern, and dental erosion concerns.
- Screen for risk factors including central obesity, smoking, family history of Barrett/esophageal cancer patterns, pregnancy, tobacco/alcohol use, age, socioeconomic constraints, and medication contributors.
- Track functional impact and response to lifestyle or medication measures over time.
- Differentiate reflux chest pain from potential cardiac ischemia presentations and escalate cardiac-rule-out workflows when indicated.
- Assess nutrition status and monitor for aspiration-related cues (wheezing, chronic cough, hoarseness) and for anemia risk when erosive disease is suspected.
- Recognize that Barrett change can be asymptomatic and may be detected during endoscopy ordered for chronic reflux symptoms.
Diagnostics
- Clinical diagnosis/PPI trial: Many clients are diagnosed by history or by symptom response to empiric proton-pump-inhibitor treatment.
- EGD escalation: Consider prompt endoscopic evaluation for alarm features (for example dysphagia/odynophagia, anemia/low red-cell indices, hematemesis, or unintended weight loss) and to evaluate erosive injury, Barrett change, stricture, or malignancy risk.
- Biopsy confirmation for Barrett change: Endoscopic tissue sampling confirms intestinal metaplasia; segment length reporting (short vs long segment) helps stratify surveillance planning.
- Ambulatory reflux monitoring: Refractory symptoms may require catheter-based LES-adjacent acid monitoring to correlate symptoms with acid exposure.
Nursing Interventions
- Reinforce individualized risk-factor reduction and symptom-trigger avoidance strategies.
- Support escalation of diagnostics and treatment when symptoms persist or warning features emerge.
- Promote adherence to long-term management plans that reduce recurrence and injury progression.
- Align care plans with pain reduction, lifestyle-modification understanding, healthy-weight progression, nutrition adequacy, and medication-adherence goals.
- Prioritize lifestyle-first management: avoid eating within about 3 hours of bedtime, elevate head of bed about 6-9 inches, and reduce common trigger foods/beverages (for example caffeine, chocolate, high-citrus, heavily spiced, or carbonated items).
- Support weight-reduction planning when obesity contributes to reflux burden.
- Encourage small, frequent meals and upright positioning during/after meals to reduce reflux burden.
- For refractory disease or intolerable medication effects, prepare clients for surgical pathways such as laparoscopic Nissen fundoplication, especially with large hiatal hernia.
- Monitor postoperative symptom changes after fundoplication, including transient bloating, dysphagia, and reduced ability to burp, while tracking overall reflux improvement.
- Teach warning monitoring for possible erosive bleeding (blood in emesis or stool) and reinforce smoking cessation, alcohol avoidance, and reduction of pressure-raising behaviors (straining, frequent bending, forceful coughing).
Pharmacology
| Drug Class | Role in GERD Care | Key Nursing Considerations |
|---|---|---|
| proton-pump-inhibitors (PPIs and H2 blockers) | First-line acid suppression when lifestyle measures are insufficient | PPIs are usually preferred for nonerosive and erosive disease control; reinforce adherence and monitoring plan. |
| proton-pump-inhibitors (H2 receptor antagonists) | Additional acid suppression option in selected symptom patterns | OTC and prescription pathways exist; verify self-medication use and response. |
| antiemetics (prokinetic therapy) | Motility support in selected refractory patterns | Metoclopramide use can be limited by long-term adverse-effect risk, so benefit-risk reassessment is essential. |
Related Concepts
- proton-pump-inhibitors - First-line acid suppression for many GERD presentations.
- digestive-system - Foundational esophageal and gastric physiology linked to reflux.
- comprehensive-abdominal-assessment - Structured symptom and red-flag assessment.