Fluid Volume Deficit Hypovolemia and Dehydration
Key Points
- Fluid volume deficit occurs when fluid loss exceeds fluid intake.
- Children younger than two years and older adults are at increased risk.
- Common causes include vomiting, diarrhea, fever with sweating, severe bleeding, excessive diuretic effect, and inadequate oral intake.
- Medication-related causes include diuretics, aldosterone-lowering antihypertensives (for example ACE inhibitors and ARBs), and laxative overuse.
- Additional high-risk groups include people with chronic disease and those with heavy heat or outdoor exposure.
- Mild deficits may respond to oral rehydration, while severe deficits often require IV fluids.
- For severe hypovolemia, rapid crystalloid infusion is first-line; albumin may be considered when crystalloid response is limited or hypoalbuminemia contributes to intravascular depletion.
- Hydration balance must account for measurable (sensible) losses and nonmeasurable (insensible) losses, especially in febrile or high-respiratory-demand states.
- Third spacing can produce intravascular hypovolemia even when total body fluid appears adequate or excessive.
Pathophysiology
Fluid volume deficit reduces effective circulating volume and can compromise perfusion of vital organs. As intravascular volume falls, compensatory mechanisms activate to preserve pressure and tissue oxygen delivery, but prolonged or severe loss can overwhelm compensation.
Early recognition is essential because progression can rapidly worsen clinical stability, especially in high-risk age groups. Severe untreated intravascular loss can progress to hypovolemic shock and cellular injury from inadequate oxygen delivery. In stable adults, most daily output is urine with the remainder as insensible skin/GI/lung losses; shifts in either pathway can rapidly create negative balance when intake does not match losses.
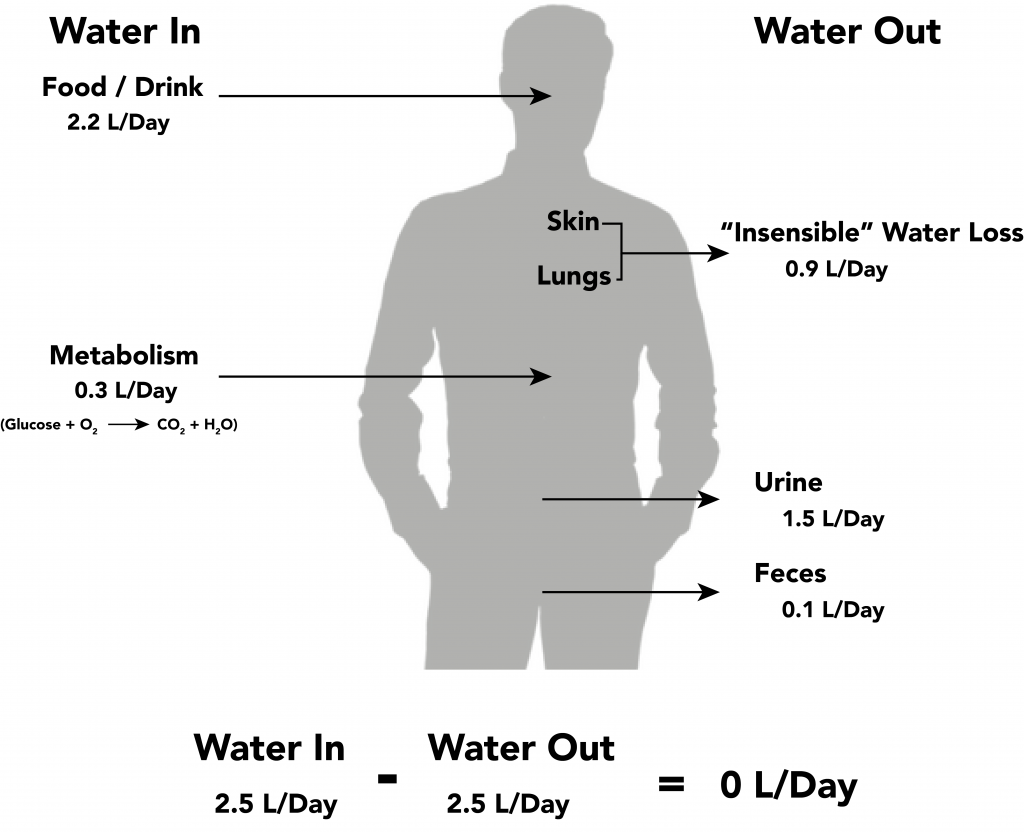 Illustration reference: OpenRN Nursing Fundamentals 2e Ch.15.2.
Illustration reference: OpenRN Nursing Fundamentals 2e Ch.15.2.
Classification
- Mild deficit: Early dehydration signs with preserved hemodynamic stability.
- Moderate deficit: Increasing clinical signs and functional decline.
- Severe deficit: Significant volume loss requiring urgent intravenous replacement.
- Third-spacing hypovolemia: Intravascular depletion from capillary leak or reduced oncotic pull with concurrent interstitial edema.
Nursing Assessment
NCLEX Focus
Prioritize high-risk populations and differentiate mild dehydration from severe volume loss requiring IV resuscitation.
- Assess recent fluid losses (vomiting, diarrhea, fever, diaphoresis) and intake history.
- Differentiate sensible losses (for example urine, emesis, diarrhea) from insensible losses (for example respiratory and skin vapor) when estimating deficit severity.
- Assess for additional intravascular loss sources, including bleeding and medication-related diuresis.
- In enteral-dependent patients, verify scheduled free-water delivery because missed doses can cause progressive dehydration and hypernatremia.
- Assess swallowing-limited intake patterns (for example severe pharyngeal pain with fever) that can rapidly reduce oral hydration.
- Assess neurologic contributors (impaired thirst signaling, reduced swallow safety, cognitive barriers) that suppress fluid intake.
- Assess classic adult dehydration cues such as thirst, dry/sticky mucous membranes, headache, dizziness, and dark concentrated urine.
- Assess additional systemic manifestations such as fatigue, confusion, muscle cramps, postural hypotension, tachycardia, chest pain, and abdominal pain.
- Assess for flat neck veins and prolonged capillary refill as intravascular depletion cues.
- Assess dehydration signs in infants and children (crying without tears, no wet diapers for 3 hours or longer, irritability or unusual drowsiness, sunken eyes, sunken fontanel).
- Assess for advanced dehydration cues such as enophthalmos, marked skin tenting, and worsening cognitive change.
- Assess older adults for subtle intake decline and delayed symptom reporting.
- Assess perfusion, urine output, and mental-status changes to gauge severity.
- Support diagnostic trend review with chemistry/electrolyte panels, CBC, and urinalysis when deficit severity or etiology is unclear.
- Trend expected hypovolemia laboratory shifts: increased hemoglobin/hematocrit, BUN/creatinine, serum osmolarity, serum sodium, and urine specific gravity.
- Flag unintentional weight loss greater than about 3 percent over 7 days as a dehydration warning pattern.
- Assess blood-pressure trend and report systolic BP below 100 mm Hg in adults (unless alternate parameters are ordered).
- Assess for orthostatic hypotension in at-risk clients (drop in systolic greater than 20 mm Hg or diastolic greater than 10 mm Hg on standing).
Nursing Interventions
- Initiate oral rehydration strategies for mild fluid deficits when safe.
- Escalate promptly for intravenous fluid therapy in severe cases.
- Use rapid isotonic crystalloid replacement as first-line therapy for severe hypovolemia/hypovolemic shock unless contraindicated by the clinical plan.
- If response to crystalloid is limited and hypoalbuminemia is a contributing factor, prepare for albumin (colloid) therapy per provider order and policy.
- Track intake, output, and response trends with frequent reassessment.
- Report urine output under 30 mL/hr or under 0.5 mL/kg/hr and monitor for progression toward kidney injury.
- Monitor for impending hypovolemic shock (rising pulse/respirations, falling BP, cold clammy skin, weak thready pulse, confusion) and escalate emergently.
- Treat persistent urine output below 30 mL/hr (or below 0.5 mL/kg/hr) over 8 hours as urgent deterioration needing escalation.
- Provide age-specific education on early dehydration warning signs.
- Coordinate follow-up to prevent recurrence after acute correction.
Delayed Recognition Risk
Late identification of worsening hypovolemia can lead to rapid deterioration and organ hypoperfusion.
Pharmacology
Fluid replacement therapy is treatment-focused; medication review should identify agents that worsen fluid loss or limit oral intake tolerance.
Clinical Judgment Application
Clinical Scenario
A toddler with two days of vomiting and diarrhea arrives with irritability, dry mucosa, and minimal urine output.
- Recognize Cues: Ongoing losses and classic dehydration findings indicate fluid deficit.
- Analyze Cues: Age-related vulnerability increases severity risk.
- Prioritize Hypotheses: Progressive hypovolemia is the priority concern.
- Generate Solutions: Determine oral rehydration viability versus IV requirement.
- Take Action: Start appropriate rehydration and monitor response closely.
- Evaluate Outcomes: Urine output, perfusion, and behavior improve toward baseline.
Related Concepts
- fluid-electrolyte-regulation-by-organs - ADH and renal responses attempt to conserve volume.
- older-adult-dehydration-risk - Older adults require focused prevention and early detection.
- pediatric-dehydration-risk - Pediatric assessment signs differ from adults.
- prevention-of-fluid-electrolyte-and-acid-base-imbalances - Prevention reduces recurrence of deficit states.
- evaluation-of-outcomes-in-fluid-electrolyte-and-acid-base-care - Structured reassessment confirms recovery.
Self-Check
- Which findings in infants suggest clinically significant dehydration?
- When is oral rehydration appropriate versus intravenous replacement?
- Why are very young and older patients at higher risk for fluid volume deficit?