Nonpharmacological Pain Management
Key Points
- Nonpharmacologic labor pain strategies improve comfort, coping, and perceived control.
- Environmental calm, movement, and supportive touch can reduce pain and anxiety during labor.
- Technique selection should be individualized to patient preference, stage of labor, and cultural context.
Pathophysiology
Labor pain is influenced by uterine and pelvic tissue stress, fetal descent dynamics, autonomic activation, and cognitive-emotional processing. Nonpharmacologic strategies reduce suffering by modulating stress response, enhancing endorphin release, improving biomechanical alignment, and strengthening coping focus.
Interventions such as positioning, hydrotherapy, breathing, and massage also influence labor mechanics and energy conservation. Their benefit is greatest when applied proactively and adjusted as labor intensity changes.
Anxiety-driven sympathetic activation (fight-or-flight response with stress-hormone release) can amplify pain perception and slow labor progression, so environmental safety and control cues are central to pain management.
Classification
- Environmental methods: Lighting control, noise reduction, music, focal points, and guided imagery.
- Comfort-touch methods: Massage, counter pressure, effleurage, cool cloths, and thermal support.
- Movement/position methods: Walking, squatting, rocking, side-lying, hands-and-knees, and pelvic tilts.
- Ball-assisted methods: Birthing-ball and peanut-ball positioning to widen hips and support rotation/descent.
- Breathing/mind-body methods: Controlled breathing, chanting, hypnosis, biofeedback, and acupressure contexts.
- Adjunct procedural methods: Sterile water injections for back-dominant labor pain in trained settings.
Nursing Assessment
NCLEX Focus
Priority assessment asks which nonpharmacologic method best matches current pain pattern, coping status, and labor stage.
- Assess pain characteristics, coping style, and preferred sensory environment.
- Use patient-reported pain tools (for example NRS or verbal descriptor scales) alongside behavioral cues and avoid appearance-only interpretation.
- Evaluate fetal and contraction status before introducing or changing comfort interventions.
- Reassess intervention effectiveness by pain report, behavior cues, and ability to rest between contractions.
- Screen for contraindications or personal boundaries (for example, touch aversion or trauma history).
- Assess whether the patient wants continuous nonmedical labor support (for example a doula) and integrate that role with nursing care.
- Screen for hydrotherapy contraindications (for example fever, vaginal bleeding, preterm status, or infectious risk) before immersion options.
- During immersion care, verify low-risk eligibility and align monitoring intervals with intermittent-auscultation standards.
Nursing Interventions
- Optimize room environment for safety and calm (dim light, reduced noise, patient-chosen music/aromatics).
- Build a patient-directed room plan early (lighting, sound, scent, focal points) and communicate it across team members to preserve continuity.
- Coach stage-appropriate movement and position changes to support descent and comfort.
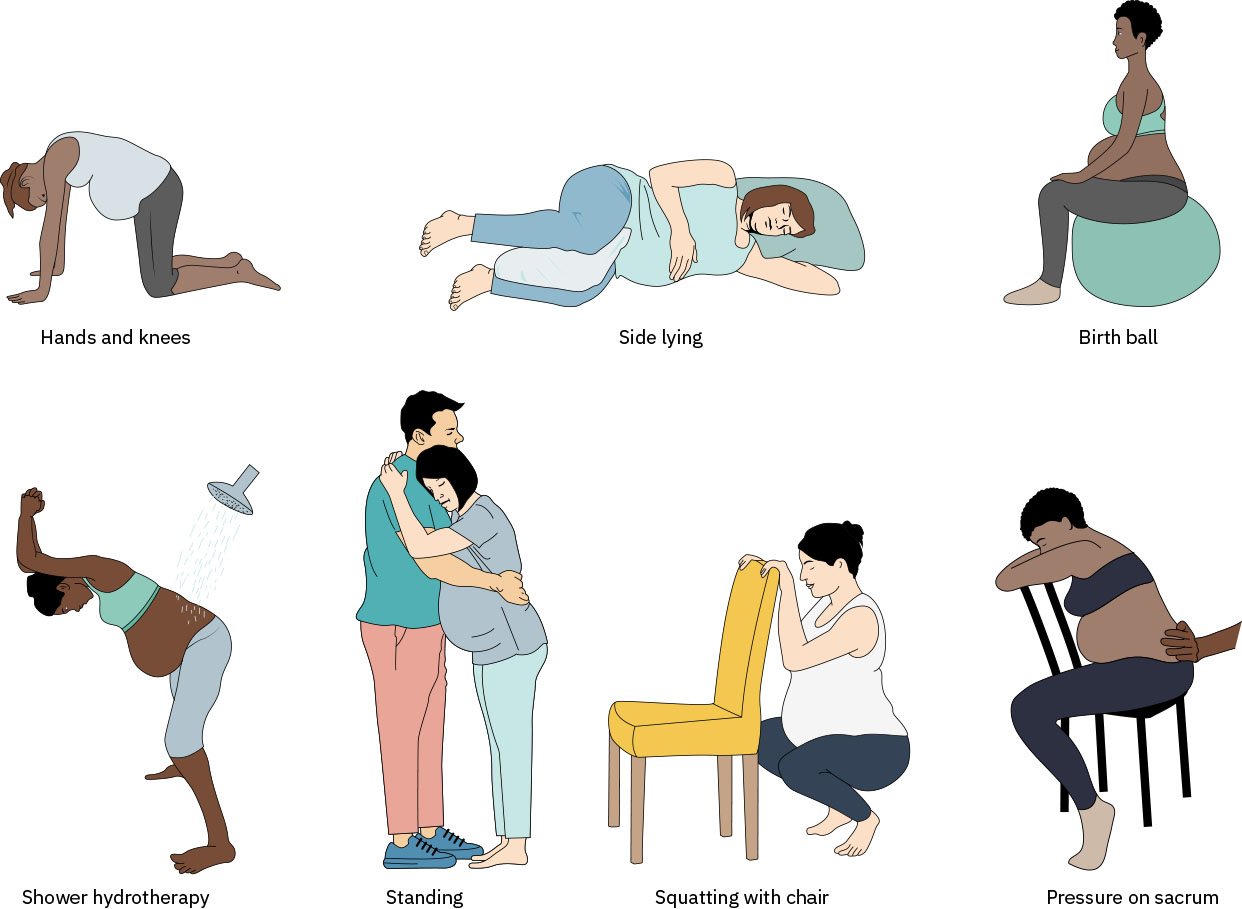 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.2.
- Use rocking-based options as tolerated (for example rocking chair, birthing ball sway, toilet sitting forward or backward when not contraindicated, or assisted side-lying hip rocking).
- Apply or guide support-person techniques such as counter pressure, hip squeeze, and effleurage.
- Use sustained hip-squeeze counter pressure for sacral/back-dominant pain and pelvic-opening support when tolerated.
- For back-dominant labor, coach hands-and-knees positioning with pelvic tilts (cat-cow pattern) to reduce sacral strain and support occiput-posterior to occiput-anterior rotation.
- In hands-and-knees intervals, pair movement with back massage, counter pressure, and hot or cold packs when preferred.
- Use side-lying positioning when back pressure is prominent or rest is needed while still promoting pelvic opening.
- Use birthing-ball and peanut-ball positioning to support hip opening and labor progress; in patients without epidural analgesia, birthing-ball use is associated with lower first-stage discomfort and shorter labor in meta-analytic evidence.
- When epidural analgesia is in place, continue position-based support (including peanut-ball side-lying setups), but counsel that outcome improvements are less consistent across studies.
- Teach and reinforce breathing patterns adaptable to early, active, and pushing phases.
- Coach breathing variants (cleansing, abdominal, chest, chanting, panting, and open or closed glottis pushing) and correct hyperventilation with slower abdominal or pursed-lip exhalation.
- During contractions, model breathing in real time with the patient when helpful and cue partners to track cleansing-breath start/end markers.
- For acupressure pathways, use only trained personnel and pregnancy-safe point sets; common labor targets include hands, feet, and ears.
- Support doula integration when present because continuous lay support is associated with lower intervention rates and higher breastfeeding and birth-satisfaction outcomes.
- Support practical comfort basics that reduce pain amplification, including hydration, scheduled voiding, and non-supine positioning.
- Offer frequent small oral fluids/ice when allowed; prolonged fasting can worsen discomfort and may contribute to ketosis/hyponatremia risk.
- Explain slowed gastrointestinal motility in labor and use small-volume intake strategies to limit nausea/vomiting burden.
- During hydrotherapy, maintain maternal-fetal surveillance using intermittent auscultation or waterproof wireless monitoring per risk status.
- In birthing-tub monitoring, place waterproof Doppler over the fetal back and assess FHR before, during, and after contractions; if waterproof equipment is unavailable, obtain intermittent checks with minimal disruption instead of full tub exit.
- For patients with epidural analgesia, encourage position changes at least every 20 to 30 minutes to support rotation, descent, and comfort.
- Reinforce childbirth-class “labor rehearsal” skills so patients and support persons can use breathing/relaxation and backup coping methods if epidural analgesia is delayed, contraindicated, or declined.
- Encourage childbirth-preparation planning that matches patient philosophy and access (hospital-based, birth-center, community, private, or online formats), including mixed-technique backup plans.
- Use cool cloths for heat, sweating, and nausea relief, and involve the support person in repeated application.
Technique-Mismatch Risk
Forcing unwanted methods can increase distress and reduce trust; comfort measures must remain patient-directed.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| labor-analgesics | Epidural, opioid, nitrous options | Nonpharmacologic methods remain useful adjuncts before and after medication use. |
| antiemetics | Nausea-management context | Support oral hydration and comfort while evaluating need for medication escalation. |
Clinical Judgment Application
Clinical Scenario
A laboring patient reports severe back pain during contractions and requests support to avoid early medication escalation.
- Recognize Cues: Increasing pain intensity, back-dominant discomfort, and preserved motivation for unmedicated coping.
- Analyze Cues: Current strategy is insufficient; combined movement and counter-pressure approach is indicated.
- Prioritize Hypotheses: Immediate priority is restoring coping effectiveness while maintaining maternal-fetal safety.
- Generate Solutions: Reassess labor status, then trial counter pressure, pelvic tilt positioning, and thermal alternation.
- Take Action: Coach support person and cycle interventions across contractions.
- Evaluate Outcomes: Pain tolerance improves, anxiety decreases, and labor participation is sustained.
Related Concepts
- birth-plans - Preference planning helps align comfort strategy before labor intensifies.
- psychosocial-adaptations-during-labor-and-birth - Emotional regulation and support affect pain perception.
- stages-of-labor - Strategy effectiveness changes across labor phases.
- pharmacological-pain-management - Integrates nonpharmacologic and pharmacologic options.
- factors-influencing-the-process-of-labor-and-birth - Position and psyche directly influence pain and progress.
Self-Check
- Which nonpharmacologic methods are most useful for back-dominant labor pain?
- How should breathing strategies be adapted from early labor to pushing?
- Which signs indicate that a comfort method should be modified or replaced?