Acute Kidney Injury
Key Points
- Acute kidney injury (AKI) is the sudden loss of kidney function over hours to days — reversible if detected and treated early.
- Three pathophysiological categories: prerenal (reduced blood flow to kidneys), intrarenal (direct kidney tissue damage), and postrenal (urinary outflow obstruction).
- Critical lab indicators: rising serum creatinine, elevated BUN, decreased GFR, and hyperkalemia — hyperkalemia is the most immediately life-threatening electrolyte implication.
- Priority nursing goal: urine output ≥30 mL/hour; oliguria (<400 mL/day) or anuria (<50 mL/day) signals severe impairment.
- Management: treat underlying cause, IV fluids (prerenal), eliminate nephrotoxins, electrolyte correction, and dialysis in severe cases.
Pathophysiology
Three Categories of AKI
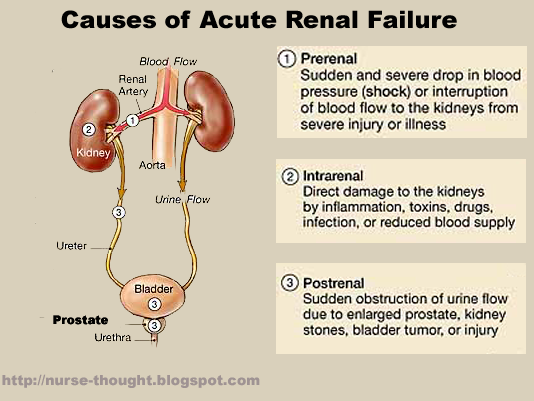 Illustration reference: OpenRN Health Alterations Ch.8.5.
Illustration reference: OpenRN Health Alterations Ch.8.5.
| Type | Mechanism | Examples |
|---|---|---|
| Prerenal | Reduced renal blood flow → decreased glomerular perfusion | Hypovolemia, hemorrhage, sepsis (sepsis), cardiogenic shock, severe heart-failure (heart failure), vascular obstruction |
| Intrarenal | Direct damage to renal tubules or nephrons | Prolonged ischemia, acute tubular necrosis from thrombotic perfusion compromise, nephrotoxic drugs (aminoglycosides, nsaids (NSAIDs), contrast media), rhabdomyolysis (myoglobin), hemolysis (hemoglobin) |
| Postrenal | Mechanical obstruction of urinary outflow → urine backflow damages kidney | benign-prostatic-hyperplasia (Benign prostatic hyperplasia) (BPH), prostate-cancer (prostate cancer), kidney stones, urethral stricture, pelvic tumors |
Prerenal causes also include severe burns and other high-volume fluid-loss states. Intrarenal injury may occur with interstitial nephritis, vasculitic or malignant-hypertension vascular injury, and selected heavy-metal toxic exposure. Some acute tubular injury episodes are transient with prompt correction, but delayed recognition can leave persistent renal dysfunction.
High-risk populations: older adults (natural decline in renal reserve), clients with CKD, diabetes, hypertension, heart failure, liver disease, autoimmune disease, dehydration, blood-loss/trauma burden, severe infection, or recent exposure to nephrotoxins or contrast dye.
Nursing Assessment
NCLEX Focus
Hyperkalemia in AKI is the priority electrolyte emergency — the kidneys cannot excrete potassium, and elevated levels cause fatal cardiac dysrhythmias. Always correlate potassium levels with ECG changes (peaked T waves, wide QRS, sine wave pattern).
Clinical manifestations by system:
| System | Manifestations |
|---|---|
| Renal | Oliguria (<30 mL/hr), anuria, uremia (elevated BUN/creatinine, uremic frost in severe cases) |
| Cardiovascular | Hypertension (fluid overload), pitting edema, heart-failure (heart failure), arrhythmias from hyperkalemia, pericarditis |
| Respiratory | Dyspnea from pulmonary edema, Kussmaul breathing (severe metabolic-acidosis (metabolic acidosis)) |
| Neurological | Confusion, asterixis (flapping tremor), peripheral neuropathy, seizures |
| GI | Nausea, vomiting, anorexia, gastritis, GI bleeding |
| Hematologic | Anemia (↓ erythropoietin), bleeding tendencies |
| Integumentary | Pruritus, pallor, dry skin, ecchymosis, uremic frost (severe) |
| Endocrine | Hyperkalemia, hyponatremia, metabolic acidosis, insulin resistance |
Priority laboratory findings:
- Serum creatinine: elevated (primary indicator)
- BUN: elevated (creatinine:BUN ratio helps identify prerenal vs intrarenal)
- GFR: decreased
- Potassium: hyperkalemia — most urgent
- Sodium: hyponatremia (dilutional)
- Arterial blood gas: metabolic acidosis (low pH, low HCO₃)
- CBC: anemia, elevated WBC if infection is cause
- Urinalysis and renal ultrasound: evaluate structural causes, obstruction, and infection contributors
Nursing Interventions
Identify and treat the underlying cause:
- Prerenal: restore circulating volume with IV fluids (isotonic crystalloids) — improve renal perfusion
- Intrarenal: identify and discontinue nephrotoxins; medications that affect renal blood flow (NSAIDs, ACE inhibitors) may need to be held
- Postrenal: relieve obstruction (urethral catheter for BPH, nephrostomy tube for stone/tumor)
Fluid and electrolyte management:
- Monitor urine output hourly — target ≥30 mL/hour; insert indwelling catheter for accurate measurement
- Hyperkalemia management: insulin + dextrose (shifts K⁺ into cells), sodium bicarbonate, kayexalate (removes K⁺ from body), cardiac monitoring — check ECG for peaked T waves, widened QRS
- For severe hyperkalemia with ECG instability, anticipate calcium-gluconate support to stabilize myocardial excitability while potassium-lowering therapy is implemented.
- Fluid restriction if oliguric to prevent fluid overload
- Sodium and fluid restriction as prescribed; dietary phosphorus and protein restriction in established AKI
Dialysis indications (severe AKI): refractory fluid overload, severe hyperkalemia, symptomatic uremia, metabolic acidosis unresponsive to treatment — hemodialysis (acute), peritoneal dialysis, or continuous renal replacement therapy (CRRT) for hemodynamically unstable clients.
- If dialysis is started, coordinate pre-treatment medication review because some medications are dialyzable or can worsen intradialytic hypotension.
Medication safety:
- Avoid or dose-adjust all renally cleared medications (digoxin, antibiotics, NSAIDs, contrast dye)
- Hold ACE inhibitors, ARBs, diuretics in prerenal AKI until volume restored
- Consult pharmacy for renal dosing adjustments
- Ensure intake/output is measured and documented accurately each shift and trended over 24 hours.
- Monitor daily weights to support fluid-balance decisions (about 1 lb gain can reflect roughly 1 L fluid accumulation), especially during dialysis care windows.
Acute Oliguria
A urine output <0.5 mL/kg/hour for more than 6 consecutive hours is a criterion for AKI and requires immediate provider notification. Do not wait for laboratory confirmation — act on clinical cues.
Related Concepts
- urinary-system — Normal glomerular filtration and nephron function disrupted in AKI.
- kidney-disease — AKI as a risk factor for CKD development; compare acute vs chronic presentations.
- potassium-balance-disorders — Hyperkalemia management as the highest-priority AKI electrolyte complication.
- peritoneal-and-hemodialysis-nursing-management — Dialysis modalities and nursing care in severe AKI.
- fluid-volume-overload-hypervolemia — Fluid overload management in oliguric AKI.
- bladder-assessment — Urine output monitoring and oliguria recognition in AKI.
Self-Check
- How do you differentiate prerenal from intrarenal AKI based on clinical history and laboratory values?
- A client with AKI has a potassium level of 6.8 mEq/L and is showing peaked T waves on the ECG. What is the priority nursing action?
- When should a nurse hold IV fluid administration for a client with AKI, and what assessment finding would guide this decision?