Mouth Throat Nose and Sinus Assessment and Abnormalities
Key Points
- Oral, pharyngeal, nasal, and sinus assessment integrates symptom interview with structured inspection/palpation.
- Swallowing pain, voice change, airway symptoms, and persistent lesions are priority cues for escalation.
- Odor/taste changes, chronic congestion, and recurrent throat inflammation can significantly affect nutrition and safety.
- Anatomy-guided technique improves discrimination between expected variation and clinically significant pathology.
- Focused questioning should capture prior diagnoses, current symptom profile, and medication/herbal use that may influence findings.
Pathophysiology
The mouth, throat, nose, and sinuses form an interconnected airway-digestive region that supports breathing, swallowing, speech, smell, and taste. Inflammation, obstruction, or infection in one area can affect the whole functional pathway.
Because airway protection and oral intake are both involved, localized pathology can rapidly influence respiratory safety, hydration, nutrition, and communication. The oral cavity includes lips, teeth, jaws, tongue, palate, uvula, and salivary structures; mastication relies heavily on masseter and temporalis function, so structural or motor change can alter chewing, speech, and intake. Dental plaque is a biofilm of retained food debris and bacteria that can demineralize enamel over time, leading to dental caries and pain-limited mastication. The pharynx includes nasopharynx (air conduction with adenoidal immune tissue), oropharynx (air-food pathway with palatine/lingual tonsils), and laryngopharynx (shared pathway to trachea/esophagus). Laryngeal and epiglottic function supports phonation and protects the airway during swallowing. Nasal structure includes external bridge/nares and internal septum, cavities, and turbinates that filter, warm, and humidify inspired air while supporting olfaction-gustation integration and resonance. Paranasal sinuses (frontal, maxillary, ethmoid, sphenoid) are mucosa-lined, air-filled spaces that lighten skull mass, influence voice quality, and contribute to mucociliary defense.
Classification
- Assessment domains: Oral mucosa/dentition/tongue, pharynx and tonsils, nasal cavity/septum/turbinates, and sinus tenderness/drainage patterns.
- Oral-structure domain: Lip/dentition alignment, jaw movement, tongue mobility, palate/uvula position, and salivary moisture pattern.
- Pharyngeal domain: Nasopharynx-oropharynx-laryngopharynx function with tonsillar and airway-protection relevance.
- Nasal-sinus domain: Septum/turbinate patency and paranasal-sinus pattern (frontal, maxillary, ethmoid, sphenoid).
- Abnormality groups: Infectious-inflammatory, structural/congenital, neoplastic warning patterns, and airway-urgent conditions.
- Symptom-risk class: Mild local irritation versus dysphagia, dyspnea, muffled voice, or progressive pain/swelling.
- Age-related sensory-change class: Older adults may show reduced smell discrimination and diminished taste sensitivity that can affect appetite, safety, and medication tolerance.
Nursing Assessment
NCLEX Focus
Prioritize airway and swallowing safety cues before lower-acuity chronic comfort complaints.
- Assess sore throat, dysphagia, hoarseness, oral pain, congestion, sinus pressure, smell/taste change, and bleeding.
- Assess for plaque-caries pattern progression (pain with chewing, visible decay, thermal sensitivity, and intake reduction due to oral discomfort).
- Assess dental-caries risk profile (for example tobacco use, diabetes, frequent high-sugar/high-carbohydrate intake, older age, and dry mouth).
- In oral-cancer suspicion, assess for loose teeth, nonhealing lip/mouth sores, red-white mucosal patches, jaw-neck lumps, mouth-ear pain, hoarseness, and chewing/swallowing/jaw-movement difficulty.
- Use focused interview prompts for prior oral/throat/nasal diagnoses (for example tooth decay, gingivitis, oral candidiasis, strep throat, tonsillitis, pharyngitis, GERD, sinusitis, rhinitis, polyps, septal deviation, nasal trauma).
- Review current medications, supplements, and herbs used for sore throat, oral lesions, congestion, or allergies.
- For active symptoms, apply PQRSTU clarification and include oral-specific questions: gum bleeding, loose/sensitive teeth, denture fit, persistent halitosis, and chewing-related intake change.
- Document lesion chronology carefully (onset, persistence, growth/bleeding change, pain pattern) and report persistent concerning findings promptly.
- Inspect oral cavity and throat for ulcers, plaques, exudate, asymmetry, mucosal color change, and lesion persistence.
- Inspect lips/teeth/gums, palate/uvula alignment, tongue mobility, and saliva quality to identify chewing/swallowing risk.
- Assess jaw movement and palpate major mastication-muscle function when chewing pain or oral-mechanics concerns are reported.
- Assess tonsillar size/exudate pattern, nasal patency and septal alignment, and sinus tenderness.
- Screen oral candidiasis risk factors in adults (for example dentures, diabetes, cancer, HIV/AIDS, recent antibiotics, inhaled corticosteroids, xerostomia, and smoking).
- Screen for poor oral-health patterns: persistent halitosis, visible decay, bleeding/receding gums, tooth sensitivity or mobility, persistent toothache, xerostomia, or persistent foul taste.
- Ask the patient to say “Ah” while using light and tongue blade to improve posterior-pharynx view and evaluate symmetric uvular rise.
- Retract lips/cheeks with gloved technique to inspect gingiva and dentition fully; remove dentures to inspect underlying mucosa.
- Evaluate for loose teeth, gum-margin ulceration/bleeding, tongue coating/lesions/motion, and salivary-gland tenderness (parotid and submandibular regions).
- Inspect external nose and use speculum with light for intranasal assessment, including drainage, septal deviation/perforation/bleeding, and turbinate congestion/polyps.
- Palpate nasal bridge/sinus regions (forehead and cheeks) for tenderness, deformity, or crepitus when fracture or sinus inflammation is suspected.
- If swallowing safety is uncertain (for example recent stroke), complete bedside swallow screening per policy before oral intake or oral medications.
- Treat failed swallow screening as
NPOuntil speech/swallow evaluation is completed. - Correlate voice resonance change and “stopped-up” quality with possible mucosal swelling or sinus-obstruction pattern.
- Differentiate common upper-airway disorders: sinusitis (acute up to 4 weeks, chronic over 12 weeks, recurrent several episodes per year), pharyngitis, tonsillitis, and epistaxis.
- Screen epistaxis contributors such as dry low-humidity conditions, digital trauma, anatomic deformity, hypertension, clotting disorders, and antiplatelet/anticoagulant use.
- Validate findings with repeat exam and symptom clarification when objective and subjective data conflict.
- Document both patient-reported data and objective findings clearly, preserving direct symptom quotes when clinically relevant.
Nursing Interventions
- Escalate red flags such as airway distress, severe dysphagia, epiglottitis-like presentation, or nonhealing suspicious lesions.
- Support ordered oral-cancer workup pathways, which may include endoscopy, tissue biopsy/brush-biopsy, HPV testing, x-ray/CT/MRI/ultrasound/PET imaging, and selected swallow studies.
- Support oral hygiene, hydration, and symptom-relief strategies while awaiting definitive treatment.
- Reinforce caries-prevention bundle: brush twice daily with fluoride toothpaste, floss daily, replace toothbrush about every 3-4 months, and pursue routine dental follow-up (commonly every 6 months).
- Reinforce fluoride and nutrition counseling (for example fluoridated water use and lower-sugar dietary pattern) plus smoking-cessation support.
- Teach sore-throat comfort measures: warm salt-water gargles (1/2 tsp salt in 1 cup water), soothing liquids, throat lozenges, humidified air, and acetaminophen when appropriate.
- Reinforce organism-specific treatment logic: most pharyngitis is viral and symptom-directed, but suspected group A streptococcal disease and bacterial tonsillitis need antibiotic adherence to reduce complications.
- Reinforce oral-candidiasis care: antifungal adherence, meticulous oral hygiene, and correction of underlying contributors.
- For patients using inhaled corticosteroids, teach rinse-and-spit mouth care after each dose to reduce recurrent oral-thrush risk.
- Refer for dental evaluation when assessment suggests possible oral disease or progressive dentition/gingival dysfunction.
- Report methamphetamine-associated oral-destruction patterns promptly and coordinate both dental referral and substance-use-treatment evaluation.
- Teach first aid for epistaxis: lean forward and pinch the lateral nose continuously up to 15 minutes while breathing through the mouth; escalate urgently for persistent bleeding or instability.
- For persistent epistaxis, prepare for stepped interventions (topical vasoconstrictor, cautery, packing/balloon) per orders and monitor hemodynamic status.
- Reinforce infection-control measures and patient education for recurrence prevention and follow-up.
- In oral-cancer treatment trajectories, prioritize airway and nutrition support, pain management, and communication adaptations (for example written communication aids after major oral procedures).
- Reinforce prevention education in at-risk profiles: tobacco and alcohol cessation, balanced diet support, and lip sun-protection counseling.
Upper-Airway Safety Risk
Progressive throat swelling or painful swallowing with respiratory change can indicate a time-sensitive airway emergency.
Common Mouth Findings
- Oral ulcer: Painful lesions on lips, tongue, gums, or buccal mucosa; consider infectious or inflammatory causes.
- Dental plaque and caries pattern: Plaque accumulation can demineralize enamel and cause cavities, oral pain, chewing difficulty, hydration/nutrition decline, and visible-esthetic distress that affects self-esteem.
- Leukoplakia: Thick white patches that can reflect chronic irritation, fungal process, or precancerous change.
- Erythroplakia: Persistent red patches with higher concern for dysplasia/malignancy, requiring prompt evaluation.
- Oral candidiasis (thrush): White plaques that can often be scraped off; more common with immunocompromise or disrupted oral flora.
- Meth mouth pattern: Severe caries, cracked/worn teeth, gum-line decay progression, xerostomia, and oral burns/lesions associated with methamphetamine exposure and delayed dental care.
- Oral cancer concern pattern: Nonhealing lesions, mucosal bleeding, color change, or oral-floor/tongue masses require prompt diagnostic follow-up.
- Oral-cancer timing cue: Any oral lesion that persists for 2 weeks or longer, especially with unusual color or bleeding, needs expedited evaluation.
- Oral-cancer treatment context: Management may include surgery, radiation, chemotherapy, and reconstructive pathways; advanced disease can require tracheostomy and feeding-tube support.
- Cleft lip / cleft palate: Congenital fusion defects that can impair feeding mechanics; cleft palate especially increases infant malnutrition risk without supportive feeding strategy and definitive repair.
- Poor oral-health cluster: Halitosis, caries, gingival bleeding/recession, dry mouth, and persistent foul taste suggest hygiene or periodontal pathology requiring follow-up.
Common Throat Findings
- Enlarged tonsils: Can reflect acute/recurrent infection or chronic inflammation.
- Tonsil groups: Palatine, pharyngeal (adenoids), lingual, and tubal tonsils.
- Tonsil grading:
0(post-tonsillectomy),1+normal,2+mild enlargement,3+moderate enlargement,4+severe enlargement.
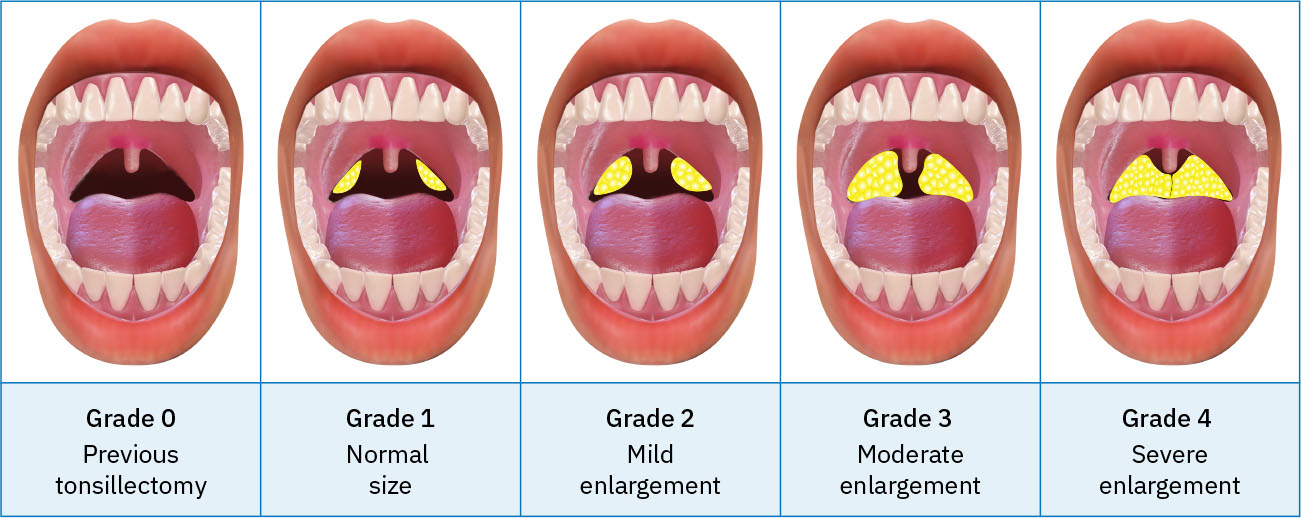 Illustration reference: OpenStax Clinical Nursing Skills Ch.22.4.
Illustration reference: OpenStax Clinical Nursing Skills Ch.22.4.
- Tonsillar exudate: White/yellow exudate may indicate bacterial pharyngotonsillar infection, including group A streptococcal disease.
- Pharyngitis pattern: Viral or bacterial; streptococcal pattern with fever, tonsillar patches, and node enlargement warrants timely antibiotic therapy to reduce complications.
- Peritonsillar abscess: Severe sore throat, dysphagia, and voice change from peritonsillar pus collection; urgent escalation needed.
- Laryngitis / epiglottitis: Hoarseness and voice loss suggest laryngeal inflammation; epiglottitis signs (painful swallowing, muffled voice, breathing difficulty) are airway emergencies.
- GERD-related throat irritation: Chronic reflux can sustain cough, hoarseness, and throat discomfort.
- Throat-cancer warning pattern: Persistent throat pain, dysphagia, or progressive voice change requires expedited workup.
- Dysphagia cue cluster: Coughing with intake, wet/gurgly voice, prolonged chewing/swallowing effort, oral leakage, retained food, or breathing difficulty after meals.
Common Nose and Sinus Findings
- Epistaxis contributors: Dry mucosa, trauma/irritants, decongestant overuse, anticoagulant/antiplatelet exposure, hypertension, polyps, and foreign bodies.
- Deviated septum: Unilateral obstruction/congestion, recurrent sinus infection, epistaxis, and sleep-disordered breathing; severe cases may require septoplasty.
- Sinusitis: Acute (up to 4 weeks), chronic (over 12 weeks), or recurrent (multiple yearly episodes) with congestion, facial pain/tenderness, and postnasal drip.
- Other nasal abnormalities: Nasal polyps, allergic/nonallergic rhinitis, fracture-related deformity, persistent obstruction/discharge, and congenital or acquired deformities.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| antibiotics | Condition-targeted agents | Confirm indication and monitor for progression despite treatment. |
| anticoagulants | Warfarin and related agents | Review bleeding-risk history and monitor persistent or recurrent epistaxis. |
| antifungal-medications | Clotrimazole, miconazole, nystatin | Commonly used for candidal lesions; reinforce course completion and oral care. |
Clinical Judgment Application
Clinical Scenario
A patient reports severe sore throat, muffled voice, painful swallowing, and increasing neck discomfort.
- Recognize Cues: Combined upper-airway and swallowing red flags.
- Analyze Cues: Pattern suggests potentially urgent airway-involved pharyngeal process.
- Prioritize Hypotheses: Immediate priority is airway safety and rapid escalation.
- Generate Solutions: Initiate urgent reassessment and avoid delays in provider evaluation.
- Take Action: Communicate objective findings clearly and implement ordered safety measures.
- Evaluate Outcomes: Early escalation prevents respiratory compromise and complication progression.
Related Concepts
- oral-perineal-and-catheter-hygiene-infection-prevention - Oral care quality affects mucosal integrity and infection risk.
- infectious-and-inflammatory-skin-conditions - Shared infectious and inflammatory pattern recognition principles.
- documenting-and-reporting-data - Objective lesion and symptom documentation improves escalation decisions.
- healthcare-associated-infections - Infection-prevention strategy supports safer care across settings.
- respiratory-system - Upper-airway anatomy and physiology provide context for sinus, pharyngeal, and nasal abnormalities.
- aspiration-pneumonia - Swallow safety screening and early aspiration-risk detection reduce pulmonary complications.
Self-Check
- Which mouth/throat findings indicate immediate airway-risk escalation?
- Why do persistent oral lesions require careful follow-up documentation?
- How can nasal and sinus findings affect broader nutrition and safety outcomes?