Newborn Resuscitation
Key Points
- The primary priority in neonatal resuscitation is establishing effective ventilation.
- Temperature control (36.5 C to 37.5 C target) is tightly linked to respiratory and metabolic outcomes.
- Positive-pressure ventilation is initiated when spontaneous breathing is absent or ineffective and heart rate remains low.
- Escalation pathways include CPAP, intubation/mechanical ventilation, and advanced therapies when hypoxemia persists.
- About 10 percent of newborns need some transition support at birth, while fewer than 1 percent require extensive resuscitation.
- During initial NRP assessment, infants who are term, breathing/crying, and have good tone receive routine care without routine suctioning even with meconium-stained fluid.
Pathophysiology
Newborn cardiac compromise generally follows respiratory failure, so delayed ventilation rapidly worsens oxygenation and perfusion. Effective lung inflation is the pivotal intervention that improves heart rate and stabilizes transition.
Hypothermia increases glucose consumption, acidosis risk, and respiratory instability. Resuscitation therefore requires simultaneous respiratory support and thermal protection.
Classification
- Initial supportive transition: Drying, stimulation, airway positioning/clearing, thermal support.
- Basic ventilatory support: Positive-pressure ventilation and oxygen titration.
- Advanced respiratory support: CPAP, intubation, conventional or high-frequency ventilation.
- Rescue-level support: Inhaled nitric oxide and ECMO for refractory cardiopulmonary failure in eligible infants.
- Initial assessment triad (first 30 seconds): Full-term status, breathing/crying effort, and muscle-tone quality to determine routine care versus resuscitation sequence.
Nursing Assessment
NCLEX Focus
Priority questions test when to escalate from routine transition support to active resuscitation.
- Assess breathing/crying effort, tone, and heart rate immediately after birth.
- Use initial 3-question triage in first 30 seconds (term gestation, effective breathing/crying, good tone/active movement) to trigger routine care or resuscitation steps.
- Trend oxygen saturation and work of breathing during and after interventions.
- Monitor for signs of persistent hypoxemia, bradycardia, or respiratory fatigue.
- Monitor thermal status continuously and correct hypothermia rapidly.
- Reassess response after each intervention step to guide escalation/de-escalation.
- In meconium-stained-fluid context, avoid routine suctioning/intubation in vigorous infants; suction only when visible obstruction or ineffective breathing suggests airway compromise.
- Review perinatal causes of impaired transition (for example cord prolapse/compression, placental abruption, uterine rupture, prolonged labor, prematurity, congenital lung/heart disorders, diaphragmatic hernia, or neonatal infection risk such as GBS pneumonia).
- Include resuscitation-risk review: limited prenatal care, gestational age below 36 weeks or at/above 41 weeks, multiple gestation, operative or emergency delivery, abnormal presentation, fetal-heart abnormality, infection, and maternal substance exposure.
Nursing Interventions
- Initiate airway positioning, drying, stimulation, and warmth without delay.
- Follow TABC sequence for initial steps (Temperature, Airway, Breathing, Circulation) during the first 30 to 60 seconds.
- Before birth, verify infant-warmer setup, preheat target temperature, and confirm oxygen/suction readiness with the neonatal-response team.
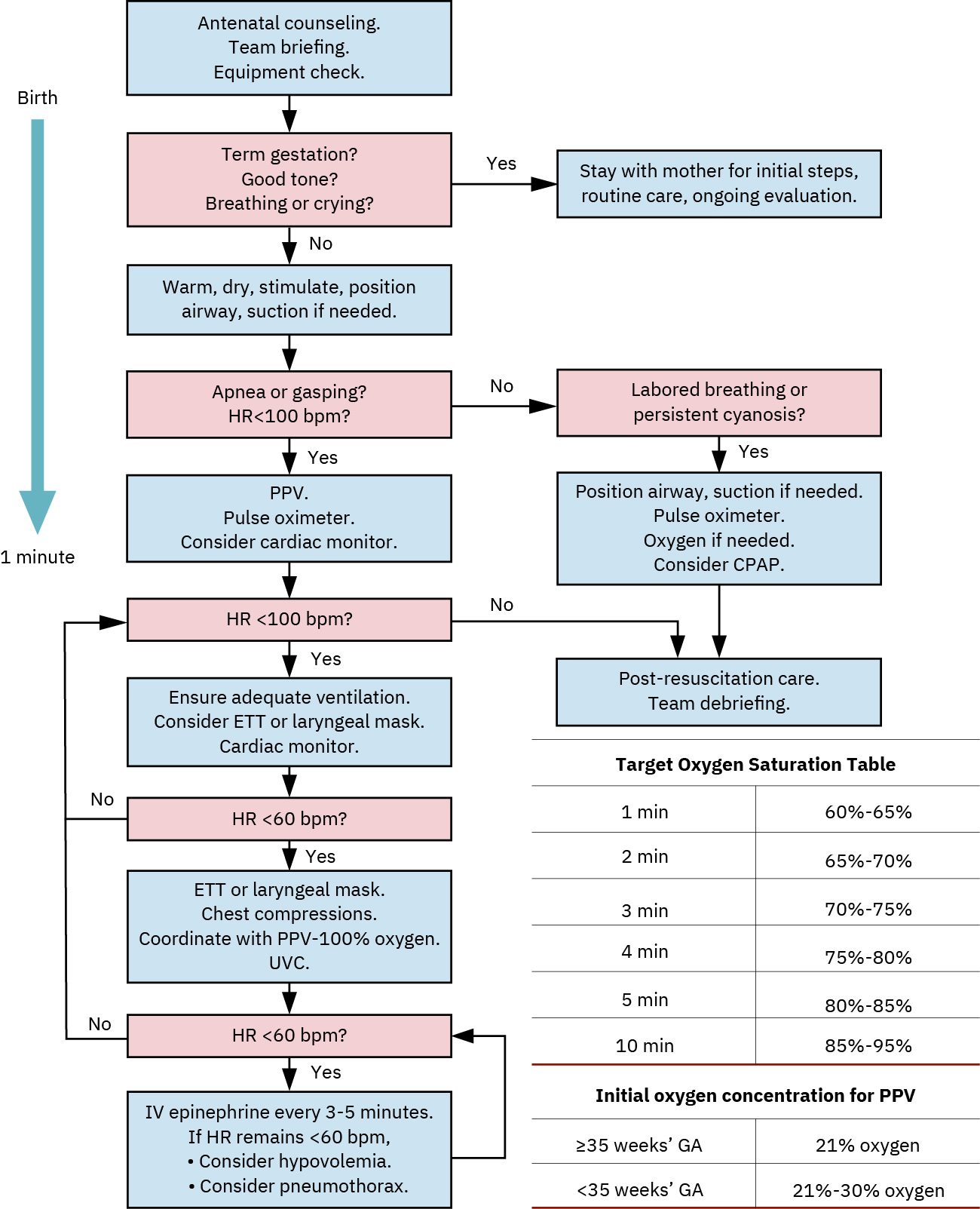 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.1.
- Start positive-pressure ventilation at protocol rate when indicated and monitor heart-rate response.
- For PPV starts, use about 21% oxygen for term infants and about 30% for preterm infants, with ventilation rate around 40 to 60 breaths/minute.
- Titrate oxygen carefully to saturation targets and avoid unnecessary hyperoxia.
- Use humidified and warmed oxygen delivery with continuous pulse oximetry to reduce cold stress and monitor response.
- If oxygen saturation remains below 92 percent or PaO2 remains below 60 mm Hg despite initial support, escalate supplemental oxygen per NRP workflow.
- If heart rate remains below 100 bpm after about 30 seconds of effective PPV, reassess mask seal/airway position/technique and escalate oxygen/advanced support per protocol.
- Begin chest compressions when heart rate remains below 60 beats per minute after effective ventilation steps.
- Use two-thumb encircling technique for compressions with 3:1 compression-to-ventilation ratio (about 90 compressions and 30 breaths per minute).
- Prepare/assist with intubation and surfactant delivery when respiratory failure persists.
- When administering surfactant, support endotracheal delivery in divided aliquots after cardiopulmonary stabilization and avoid routine suctioning for about 1 hour unless airway obstruction is suspected.
- Escalate to mechanical ventilation when hypoxemia or hypercapnia persists, including cases with apnea/bradycardia, asphyxia, sepsis, meconium aspiration syndrome, or respiratory distress syndrome.
- Consider high-frequency ventilation when available to deliver lower-pressure breaths and reduce barotrauma risk.
- Prepare and administer epinephrine when bradycardia persists despite ventilation/compressions per protocol and order set.
- In advanced neonatal resuscitation pathways, anticipate epinephrine dosing around 0.01 to 0.03 mg/kg when heart rate remains below 60 bpm despite effective ventilation/compressions.
- If shock or blood loss is suspected, support rapid IV fluid/blood-product resuscitation per team orders.
- Coordinate multidisciplinary escalation for nitric oxide or ECMO candidacy in refractory cases, and recognize ECMO anticoagulation raises intracranial bleeding risk and is generally not used below 34 weeks’ gestation.
- After successful resuscitation, continue close monitoring of HR/RR/SpO2, maintain normothermia (about 36.5 C to 37.5 C), and transfer to NICU when ongoing support is needed.
Ventilation Delay
Delayed initiation of effective ventilation significantly increases risk of severe morbidity and death in compromised newborns.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| surfactants | Beractant (Survanta) context | Used in surfactant-deficient lungs via endotracheal route; monitor for desaturation, bradycardia, blood-pressure changes, and severe complications such as pulmonary hemorrhage or PDA. |
| preterm-newborn (inhaled-nitric-oxide) | iNO context | Pulmonary vasodilation support for selected severe hypoxemia/pulmonary hypertension pathways. |
| oxygen-therapy | Supplemental oxygen context | Deliver humidified/warmed oxygen with close saturation monitoring and titration. |
| epinephrine | NRP medication context | Reserve for persistent severe bradycardia after ventilation/compressions; verify dose/route rapidly. |
Clinical Judgment Application
Clinical Scenario
A newborn at 1 minute remains apneic with poor tone and heart rate under 100 bpm despite stimulation and airway repositioning.
- Recognize Cues: Persistent apnea and bradycardia indicate failed spontaneous transition.
- Analyze Cues: Ventilatory failure is primary cause of ongoing instability.
- Prioritize Hypotheses: Immediate priority is effective ventilation and thermal stabilization.
- Generate Solutions: Begin PPV, apply monitoring, reassess heart rate, and escalate respiratory support if inadequate response.
- Take Action: Implement protocolized resuscitation sequence and call neonatal team support.
- Evaluate Outcomes: Heart rate rises and respiratory effort improves, or advanced support pathway is activated.
Related Concepts
- apgar-scoring - Guides urgency of transition support and repeated reassessment.
- physiological-adaptation-and-transition - Underlying physiology explains resuscitation priorities.
- neutral-thermal-environment - Thermal management is integral to successful resuscitation.
- preterm-newborn - Prematurity substantially increases need for respiratory intervention.
- birth-related-complications - Birth trauma may precipitate immediate resuscitation needs.
Self-Check
- Why is ventilation prioritized over other interventions in most neonatal resuscitation events?
- Which findings indicate the need to escalate from PPV to advanced respiratory support?
- How does hypothermia worsen resuscitation outcomes in newborns?