Placental Abruption
Key Points
- Placental abruption is the premature separation of the placenta from the uterine lining, which is an obstetric emergency.
- Severity ranges from partial to complete abruption; complete separation can lead to fetal demise and maternal death from hemorrhage.
- Classic presentation: painful vaginal bleeding, uterine tenderness, and rigid (“board-like”) abdomen.
- Risk factors include preeclampsia, chronic hypertension, smoking, trauma, cocaine use, and prior abruption.
Pathophysiology
Placental abruption occurs when the placenta separates from the uterine wall before delivery, disrupting blood flow between the parent and fetus. Separation may result from rupture of the maternal blood vessels in the decidua basalis, forming a retroplacental hematoma that progressively enlarges and detaches more of the placenta. The degree of hemorrhage depends on the extent of separation — partial abruption may present with concealed or revealed bleeding, while complete abruption results in massive hemorrhage with fetal hypoxia and death. Abruption is a known complication of preeclampsia, eclampsia, and DIC.
Classification
- Partial abruption: A portion of the placenta separates; fetal compromise varies with the degree of detachment.
- Complete abruption: The entire placenta separates from the uterine wall; constitutes a life-threatening emergency for both parent and fetus.
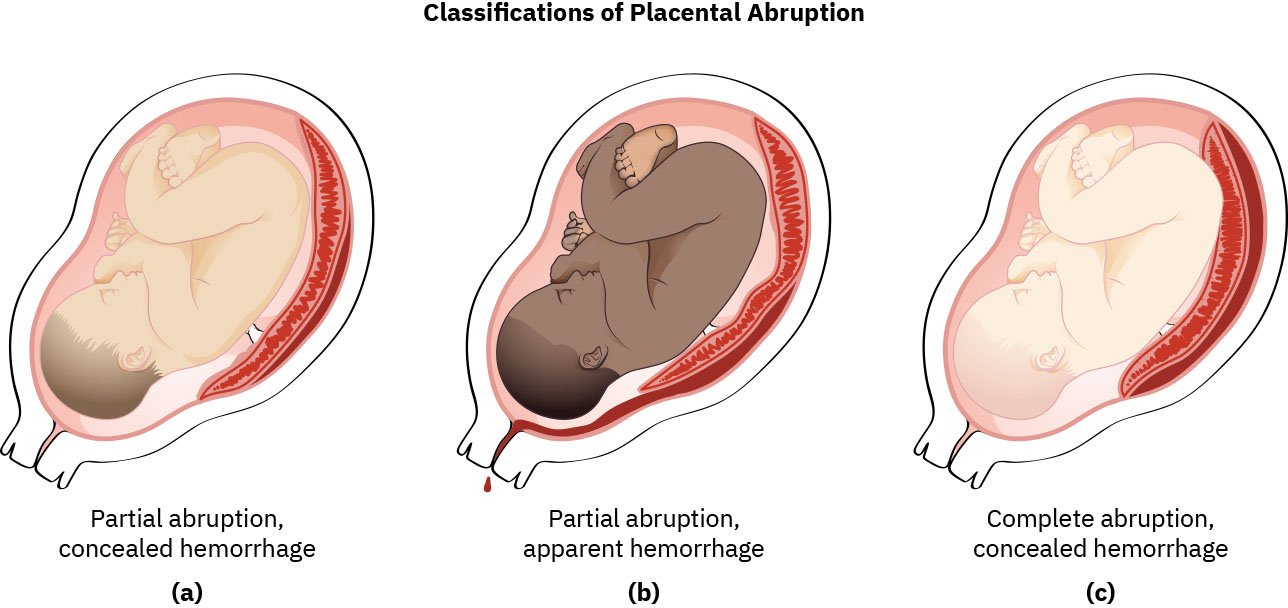 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.12.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.12.2.
Clinical Manifestations
- Painful vaginal bleeding (dark red); however, bleeding may be concealed in some cases.
- Abdominal pain and uterine tenderness, often sudden onset.
- Rigid, board-like uterus with increased uterine tone.
- Prolonged uterine contraction pattern with limited or absent resting tone between contractions.
- Signs of maternal hemorrhagic shock: tachycardia, hypotension, pallor, diaphoresis.
- Fetal heart rate abnormalities: late decelerations, bradycardia, or absent variability.
- Uterine contractions may be frequent and hypertonus.
- Back pain.
Nursing Assessment
NCLEX Focus
Differentiate placental abruption (painful, dark bleeding, board-like uterus) from placenta previa (painless, bright red bleeding, soft uterus). This is a high-yield comparison on NCLEX.
- Assess amount and character of vaginal bleeding (dark red vs. bright red, with or without pain).
- Palpate uterus for rigidity, tenderness, and increased tone.
- Monitor maternal vital signs for signs of hemorrhagic shock.
- Apply continuous electronic fetal monitoring to assess fetal heart rate patterns.
- Monitor laboratory values: CBC, coagulation studies (PT, PTT, fibrinogen, D-dimer), type and crossmatch.
- Assess for signs of DIC: oozing from venipuncture sites, petechiae, prolonged clotting times.
Nursing Interventions
- Maintain large-bore IV access (two sites); initiate aggressive fluid resuscitation with isotonic crystalloids.
- Administer blood products as ordered (packed RBCs, fresh frozen plasma, cryoprecipitate for DIC).
- Position patient in left lateral position to optimize uteroplacental perfusion.
- Prepare for emergent cesarean delivery if fetal distress is present or abruption is severe.
- Administer magnesium-sulfate if preeclampsia/eclampsia is concurrent.
- Monitor strict intake and output; assess for decreased urine output as a sign of hypovolemia or renal compromise.
- Provide emotional support to the patient and family during the emergency.
Concealed Hemorrhage
External bleeding may not reflect the true volume of blood loss. A rigid, enlarging uterus with fetal distress but minimal vaginal bleeding suggests concealed retroplacental hemorrhage.
Related Concepts
- preeclampsia — Major risk factor and associated condition.
- placenta-previa — Key differential diagnosis for antepartum bleeding.
- disseminated-intravascular-coagulation-in-pregnancy — Life-threatening complication of severe abruption.
- Hemorrhagic Shock — Consequence of significant maternal blood loss.
- fetal-heart-rate-and-contraction-patterns — Essential for detecting fetal compromise.
Self-Check
- How does the clinical presentation of placental abruption differ from placenta previa?
- Why can external bleeding underestimate true blood loss in placental abruption?
- What laboratory findings suggest the development of DIC in a patient with abruption?