Neutral Thermal Environment
Key Points
- A neutral thermal environment for newborns is maintained around 36.5 C to 37.0 C during transition.
- Newborns lose heat by evaporation, convection, conduction, and radiation.
- Cold stress can trigger hypoglycemia, respiratory changes, irritability, and increased metabolic demand.
- Prompt rewarming, reassessment, and escalation prevent progression to severe instability.
- Temperature thresholds guide action: mild hypothermia/cold stress below 36.5 C (above 35.5 C), moderate 32.0 to 34.9 C, severe below 32.0 C, and hyperthermia above 37.5 C.
- Ten-step warm-chain workflows remain high-yield for preventing avoidable heat loss, especially in low-resource settings.
Pathophysiology
Newborns have high surface-area-to-mass ratio, thin skin, limited brown fat reserves, and no effective shivering response. These factors make them highly vulnerable to environmental heat loss during the immediate postbirth period.
Delivery-room ambient temperature and evaporation of birth fluid can lower newborn temperature by about 2 C during the first 30 minutes if heat-loss prevention is delayed.
When temperature drops, the newborn increases oxygen and glucose use through nonshivering thermogenesis. Persistent cold stress can deplete energy stores, worsen respiratory effort, and impair adaptation. Severe uncorrected cold stress can reduce surfactant performance, worsen pulmonary blood-flow mismatch, and increase risk of serious complications.
Classification
- Evaporative heat loss: Fluid on skin converts to vapor and removes heat.
- Convective heat loss: Cool moving air removes body heat.
- Conductive heat loss: Direct contact with cool surfaces draws heat away.
- Radiant heat loss: Nearby cold objects/walls pull heat without direct contact.
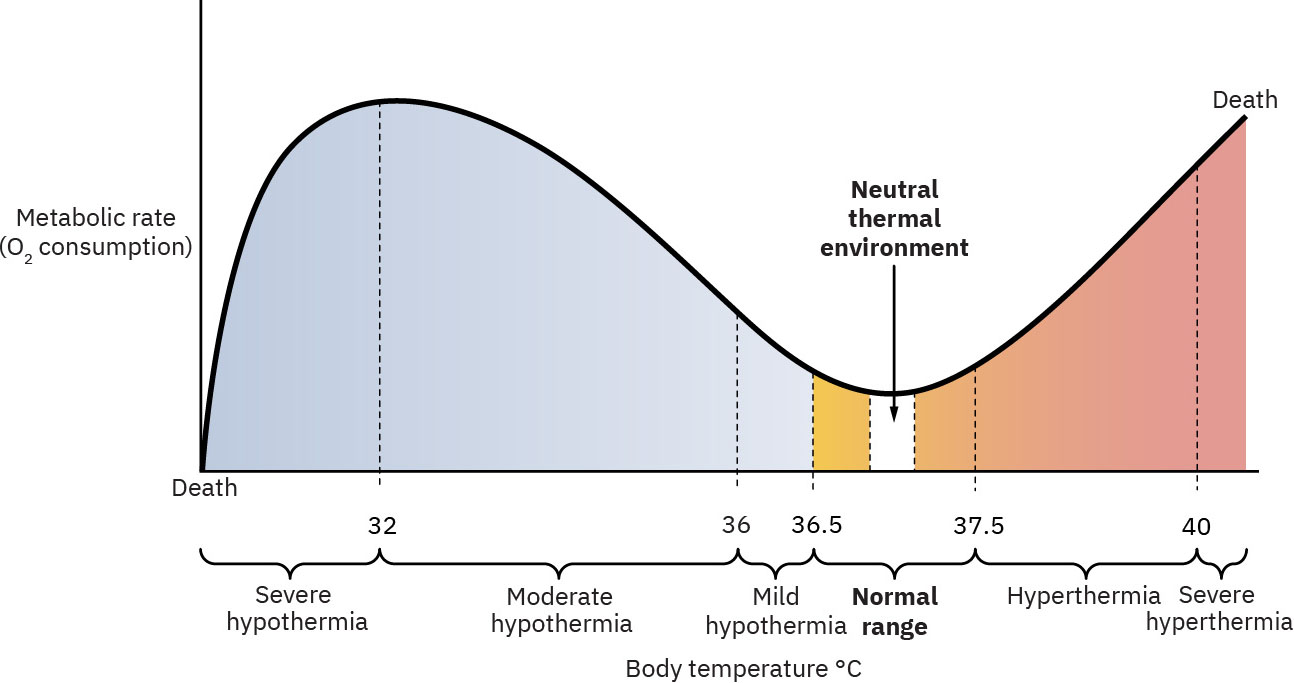 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.3.
-
Hypothermia severity: Mild/cold stress (35.5 C to under 36.5 C), moderate (32.0 C to 34.9 C), severe (under 32.0 C).
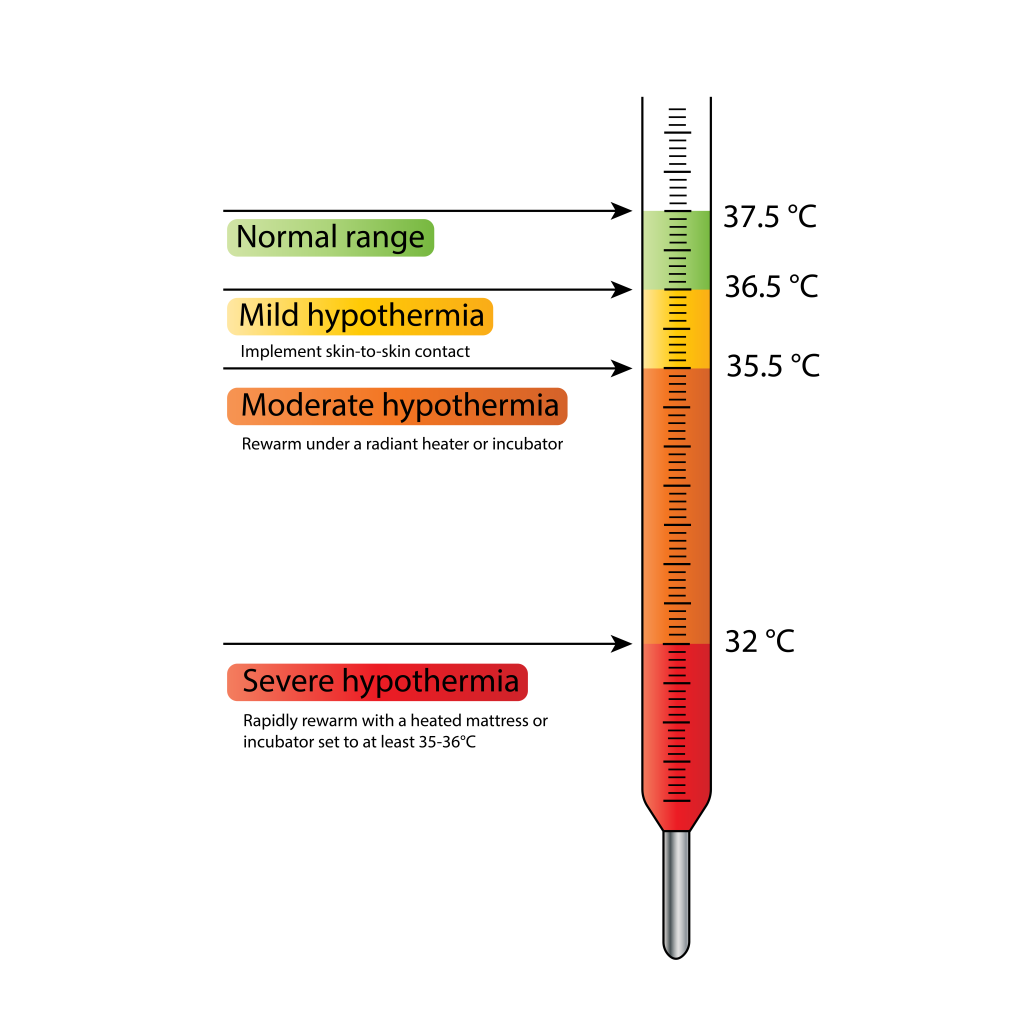 Illustration reference: OpenRN Nursing Health Promotion Ch.12.3.
Illustration reference: OpenRN Nursing Health Promotion Ch.12.3. -
Hyperthermia state: Temperature above 37.5 C, often due to overheating environment/clothing/bedding.
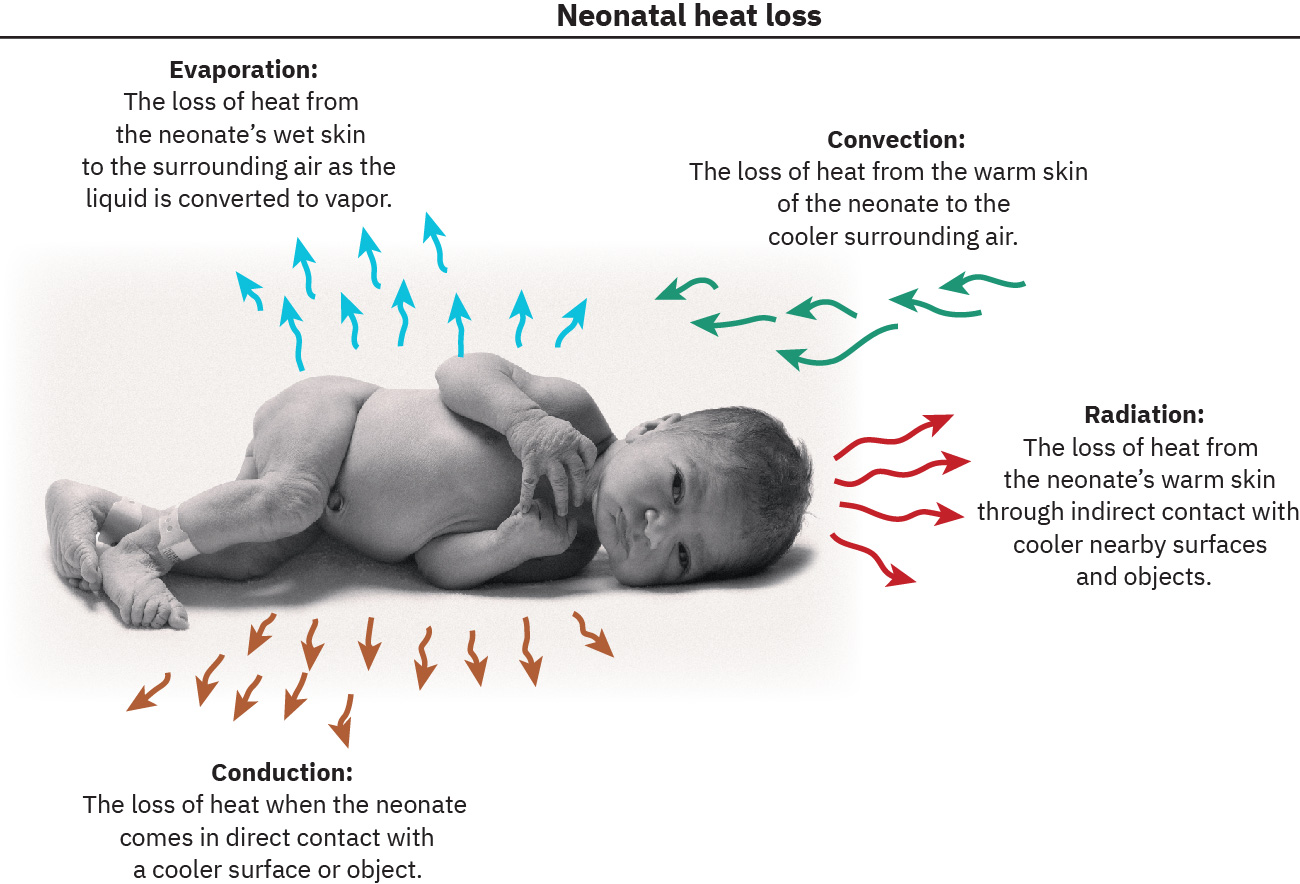 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.3.
Nursing Assessment
NCLEX Focus
Priority items test whether the nurse identifies subtle early cold-stress cues before severe deterioration.
- Monitor axillary temperature trends and frequency of instability episodes.
- Assess for early cold-stress cues: irritability, altered respiratory pattern, jitteriness, poor feeding.
- In mild hypothermia, assess for cool extremities, weak cry, low activity, poor feeding, and tachypnea/labored breathing.
- In moderate/severe hypothermia, assess for bradycardia, decreased respiratory depth/rate, worsening hypoglycemia, and acidosis risk.
- Check blood glucose in at-risk or symptomatic infants because hypothermia and hypoglycemia often coexist.
- Assess environment for preventable heat-loss exposures (wet linens, drafts, cold surfaces, nearby windows).
- Assess overheating risk factors (overbundling, prone sleep, bed-sharing, hot room) because hyperthermia may increase SIDS risk.
- In early transition, correlate thermal findings with expected reactivity phases; persistent tachycardia, recurrent apnea, or fixed bradycardia with hypothermia are abnormal.
- Reassess response within 30 minutes after thermal interventions.
Nursing Interventions
- Dry newborn promptly after birth/bathing and apply hat, warm blankets, and skin-to-skin care.
- Use warm-chain prevention: dry immediately, replace wet linens promptly, begin skin-to-skin, and avoid drafts/fan airflow.
- Align room-temperature strategy to context: many warm-chain protocols target delivery-room temperature at least 25 C (77 F), while term/postterm nursery environmental targets may be lower based on local policy and monitoring.
- Maintain initial skin-to-skin for about 60 to 90 minutes when stable and continue as a first-line rewarming strategy for mild hypothermia.
- Use radiant warmer or incubator when skin-to-skin is insufficient to restore normothermia.
- For moderate/severe hypothermia, use radiant warmer/incubator around 35 to 36 C; if warmer unavailable, continue skin-to-skin in a room at least 77 F.
- Support early feeding (breast or formula) to provide calories for thermogenesis.
- Delay routine weighing for several hours and delay bathing until thermal stability is established; many protocols delay at least 6 to 24 hours, with longer delay when instability risk is high.
- Keep mother-infant dyad together and ensure warm transport between care areas.
- Follow warm-chain principles across transport, handling, and room environment.
- Minimize unnecessary exposure and cluster care to reduce repeated heat loss.
- During active rewarming pathways, trend temperature more frequently (for example hourly in early high-risk windows) and resume routine cadence once stable.
- Escalate for persistent low temperature or concurrent respiratory distress and neurologic changes.
Persistent Hypothermia
Temperature below 36.5 C after about 30 minutes of active rewarming, or any moderate/severe hypothermia with cardiorespiratory compromise, requires urgent provider/NICU notification.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| intravenous-fluid-categories-tonicity-and-infusion-regulation (dextrose) | Point-of-care hypoglycemia treatment context | Treat low glucose promptly when cold stress increases metabolic demand. |
| oxygen-therapy | Supplemental oxygen context | May be needed if cold stress is accompanied by respiratory compromise. |
Clinical Judgment Application
Clinical Scenario
A newborn at 3 hours of life has axillary temperature below target, jitteriness, and mild nasal flaring after prolonged uncovered handling.
- Recognize Cues: Temperature instability with early metabolic/respiratory stress signs.
- Analyze Cues: Environmental heat loss likely triggered cold stress with possible hypoglycemia risk.
- Prioritize Hypotheses: Immediate priority is rewarming and metabolic stabilization.
- Generate Solutions: Initiate warm-chain actions, radiant warmer support, glucose check, and repeat focused assessment.
- Take Action: Implement rewarming and notify provider if instability persists.
- Evaluate Outcomes: Temperature normalizes and respiratory/neurologic signs improve.
Related Concepts
- physiological-adaptation-and-transition - Thermal stability is critical to successful neonatal adaptation.
- physical-assessment-of-the-newborn - Vital-sign and behavior findings detect early cold-stress progression.
- care-of-common-problems-in-the-newborn - Cold stress increases glucose consumption and hypoglycemia risk.
- apgar-scoring - Immediate transition scoring often links with thermoregulation priorities.
- care-of-common-problems-in-the-newborn - Routine care workflows should preserve thermal stability.
Self-Check
- What are the four mechanisms of neonatal heat loss and one prevention strategy for each?
- Why does cold stress increase risk of hypoglycemia?
- Which findings indicate that independent nursing interventions are no longer sufficient?