Physiological Adaptation and Transition
Key Points
- Transition to extrauterine life requires rapid closure/reversal of fetal shunts and initiation of effective lung function.
- Key circulatory structures include the ductus venosus, foramen ovale, and ductus arteriosus.
- Respiratory adaptation failure causes early neonatal distress syndromes requiring prompt recognition.
- Newborn transition follows predictable reactivity phases, and persistent abnormalities warrant escalation.
- Typical closure timing varies: foramen ovale functionally closes in early hours, ductus arteriosus functionally constricts over hours to days (anatomic closure over weeks to months), and ductus venosus narrows in early days with later anatomic closure.
- Preductal oxygen saturation normally rises over the first 10 minutes after birth (about 60 to 65 percent at 1 minute to about 85 to 95 percent at 10 minutes).
Pathophysiology
At birth, placental circulation ceases and lung expansion lowers pulmonary vascular resistance. Left-sided cardiac pressures rise, fetal shunts close functionally, and blood flow shifts to the mature neonatal circulation pattern.
First breaths clear lung fluid, expand alveoli, and support oxygen exchange. If this sequence is delayed or disrupted, hypoxemia, acidosis, and respiratory distress may occur. Labor-associated catecholamine surge helps switch fetal lung epithelium toward fluid reabsorption to support early air entry.
Before birth, oxygen and nutrients arrive from the placenta through the umbilical vein. Blood largely bypasses the fetal liver via the ductus venosus, then bypasses most pulmonary flow through the foramen ovale (right atrium to left atrium) and ductus arteriosus (pulmonary artery to aorta). Two umbilical arteries return deoxygenated blood and wastes to the placenta.
After cord clamping, systemic vascular resistance rises and right-to-left shunt flow rapidly declines. With first breaths and alveolar oxygenation, pulmonary vascular resistance falls, left-atrial filling rises, and pressure reversal supports functional foramen ovale closure in early hours (often about 1 to 2 hours). Ductus venosus flow falls with loss of umbilical-vein flow; narrowing begins in the first days, often closing functionally within the first week in term newborns, with later anatomic closure. With first breaths and falling pulmonary vascular resistance, ductus arteriosus flow decreases; functional constriction/closure occurs over hours to days, while anatomic closure extends over weeks to months.
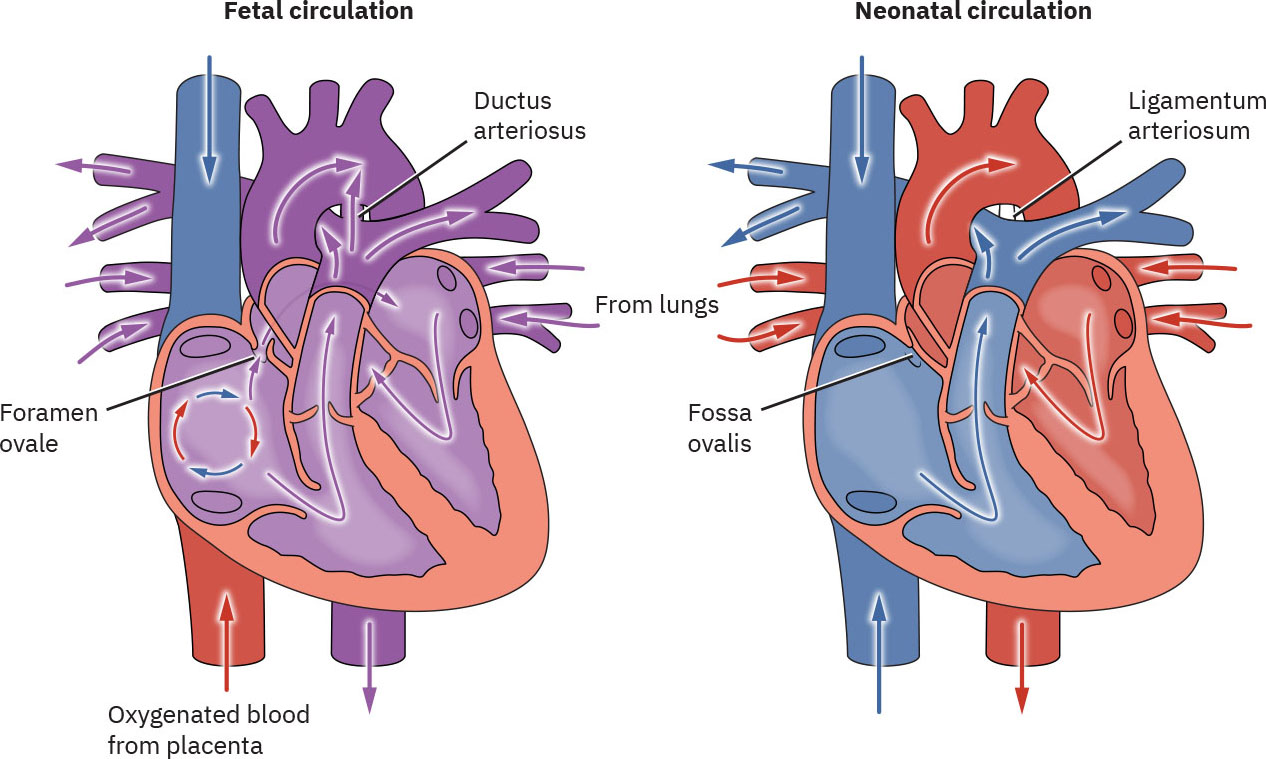 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.22.2.
Post-transition remnants are expected: foramen ovale closure leaves the fossa ovalis, ductus arteriosus becomes the ligamentum arteriosum, and ductus venosus becomes the ligamentum venosum.
Classification
- Circulatory adaptation: Functional closure of foramen ovale and ductus arteriosus with systemic-pulmonary pressure reversal.
- Fetal-circulation baseline: Placental oxygenation with umbilical-vein inflow and shunt-dependent bypass of liver/lungs before birth.
- Neonatal hemodynamic profile: Limited ventricular compliance and immature myocardium reduce ability to raise stroke volume during stress.
- Respiratory adaptation: Airway fluid clearance, surfactant-supported alveolar expansion, and effective gas exchange.
- Early respiratory-distress patterns: MAS, TTN, RDS, and PPHN as common immediate-transition differentials.
- Behavioral transition phases: First reactivity, decreased responsiveness (about 30 minutes to 2 hours), and second reactivity (about 2 to 8 hours).
- Abnormal transition patterns: Persistent cyanosis, prolonged respiratory distress, hemodynamic instability, or unusual neurologic behavior.
Nursing Assessment
NCLEX Focus
Priority questions test recognition of expected early transition findings versus persistent abnormalities needing escalation.
- Monitor cardiopulmonary status for tachypnea, grunting, retractions, flaring, persistent cyanosis, and oxygen saturation trends.
- Assess for signs associated with persistent shunt pathology (murmur, tachycardia, hypoxia, perfusion changes).
- Track expected preductal oxygen-saturation progression over first 10 minutes post birth (about 60 to 65 percent at 1 minute, 80 to 85 percent by 5 minutes, and 85 to 95 percent by 10 minutes).
- In newborns to about 6 months, interpret perfusion changes with the understanding that cardiac output is predominantly heart-rate dependent.
- Monitor for bradycardia as a high-risk cue because limited stroke-volume reserve can rapidly reduce cardiac output.
- In possible shock states, do not rely on blood pressure alone because hypotension is often a late decompensation finding in neonates.
- Assess glucose, calcium, temperature, oxygenation, and acid-base stressors because hypoglycemia, hypocalcemia, hypoxia, and acidosis can impair neonatal contractility.
- Assess transition-phase behavior and feeding readiness across first hours.
- During decreased-responsiveness phase, expected findings include lower activity with preserved perfusion and reduced response to stimuli; prolonged depression is abnormal.
- During second-reactivity phase, anticipate brief return of alertness/hunger cues and possible transient mucus gagging/choking while airway secretions clear.
- Identify risk history (prematurity, meconium exposure, maternal disease/medications, birth complications).
- In suspected PDA, recognize continuous machine-like murmur with tachycardia and bounding pulses as escalation cues.
- In suspected PFO, recognize that many neonatal findings are transient/benign but still require provider notification when murmur is heard.
- Treat persistent transition red flags as urgent: SpO2 below 90 percent after first hour, apnea longer than 20 seconds with bradycardia, marked pallor, capillary refill over 3 seconds, or ongoing severe respiratory effort.
Nursing Interventions
- Support airway/ventilation with positioning, suctioning, and escalation to positive-pressure ventilation as indicated.
- Maintain thermoregulation to reduce metabolic demand during respiratory/circulatory adaptation.
- In unstable transition, maintain continuous temperature monitoring and keep core temperature in normothermic range (commonly about 36.5 C to 37.4 C).
- Use pulse oximetry and serial reassessment to guide oxygen and resuscitation decisions.
- When clinically feasible, support delayed cord clamping for about 30 to 60 seconds to improve early neonatal hemoglobin and circulatory transition.
- Avoid unmonitored rapid fluid loading in neonates because low-compliance ventricles are vulnerable to overdistention and fluid-overload heart-failure patterns.
- Escalate persistent tachycardia, bradycardia, weak perfusion, or feeding decline even when blood pressure appears within age range.
- Support metabolic stability (temperature, glucose, and calcium control) to reduce secondary myocardial dysfunction during transition.
- Report persistent murmurs or poor perfusion findings for provider evaluation.
- Coordinate neonatal team involvement early for preterm or high-risk transition.
Persistent Distress
Ongoing cyanosis, apnea, severe retractions, or poor perfusion after initial transition period requires immediate advanced evaluation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| vitamin-k | Phytonadione | Routine prophylaxis reduces early and late vitamin-K-deficiency bleeding risk. |
| oxygen-therapy | Supplemental oxygen context | Use saturation targets and avoid unnecessary hyperoxia during transition support. |
Clinical Judgment Application
Clinical Scenario
A late-preterm newborn has persistent tachypnea, nasal flaring, low saturation trend, and poor feeding during the first hour of life.
- Recognize Cues: Sustained respiratory work and suboptimal oxygenation beyond expected transitional variability.
- Analyze Cues: Adaptation failure with possible respiratory distress syndrome pathway.
- Prioritize Hypotheses: Immediate priority is oxygenation and ventilation support while identifying cause.
- Generate Solutions: Airway positioning, pulse oximetry-guided oxygen, thermal support, and neonatal-team escalation.
- Take Action: Implement protocolized support and frequent reassessment.
- Evaluate Outcomes: Work of breathing and oxygenation improve or infant transfers for higher-level care.
Related Concepts
- apgar-scoring - Rapid snapshot of transition effectiveness immediately after birth.
- neutral-thermal-environment - Thermoregulation stability supports cardiopulmonary adaptation.
- congenital-heart-defects-acyanotic-and-cyanotic-patterns - Structural postnatal circulation defects that alter expected transition trajectory.
- acute-respiratory-distress-syndrome - Major cause of failed respiratory transition in preterm newborns.
- preterm-newborn - Common early tachypnea pattern linked to delayed lung-fluid clearance.
- preterm-newborn - Severe adaptation failure with refractory hypoxemia.
Self-Check
- Which hemodynamic changes close fetal shunts after birth?
- Which findings suggest normal transition versus evolving respiratory failure?
- Why does thermoregulation directly affect successful cardiopulmonary transition?