Fetal Lie, Presentation, Position, and Station
Key Points
- Fetal orientation determines how efficiently labor power can translate into cervical change and descent.
- Assessment combines abdominal palpation (Leopold maneuvers), vaginal landmarks, and ultrasound confirmation when needed.
- Longitudinal cephalic positions are usually most favorable for vaginal birth, while transverse lie is not compatible with routine vaginal delivery.
- Station documents fetal descent relative to the ischial spines, with
0indicating engagement.- Occiput posterior is a common cephalic malposition (about 15 to 30 percent of cephalic births), and breech occurs in about 3 to 4 percent of labors.
Pathophysiology
Fetal passage through the maternal pelvis requires alignment between the fetal presenting part and pelvic dimensions. During labor, skull molding and rotational movements reduce effective fetal diameters and support descent; unfused sutures and fontanelles allow adaptive molding without lasting injury.
When lie, presentation, or position is unfavorable, labor may prolong, descent can stall, and fetal stress risk increases. Accurate assessment helps nurses distinguish expected variation from malposition requiring escalation. Fetal lie specifically describes fetal long-axis relationship to the maternal long axis. At term, most fetuses (more than 95 percent) are longitudinal; persistent non-longitudinal lie near term raises procedural-delivery risk.
Classification
- Lie: Longitudinal versus non-longitudinal (oblique or transverse). Transverse lie is perpendicular to maternal axis (often described as back-up or back-down) and is generally incompatible with routine vaginal birth at term.
- Oblique lie pattern: Axis sits between longitudinal and transverse; some convert to longitudinal with active-labor contraction pressure, but persistence can slow progress when the presenting part does not apply effective cervical pressure.
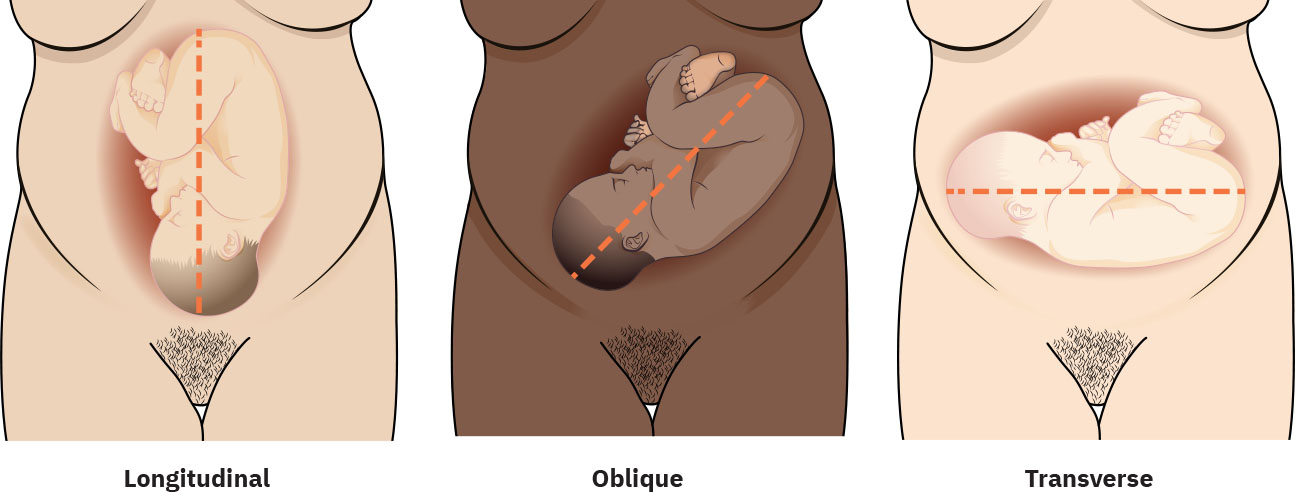 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.4.
- Presentation: Cephalic, breech, or shoulder.
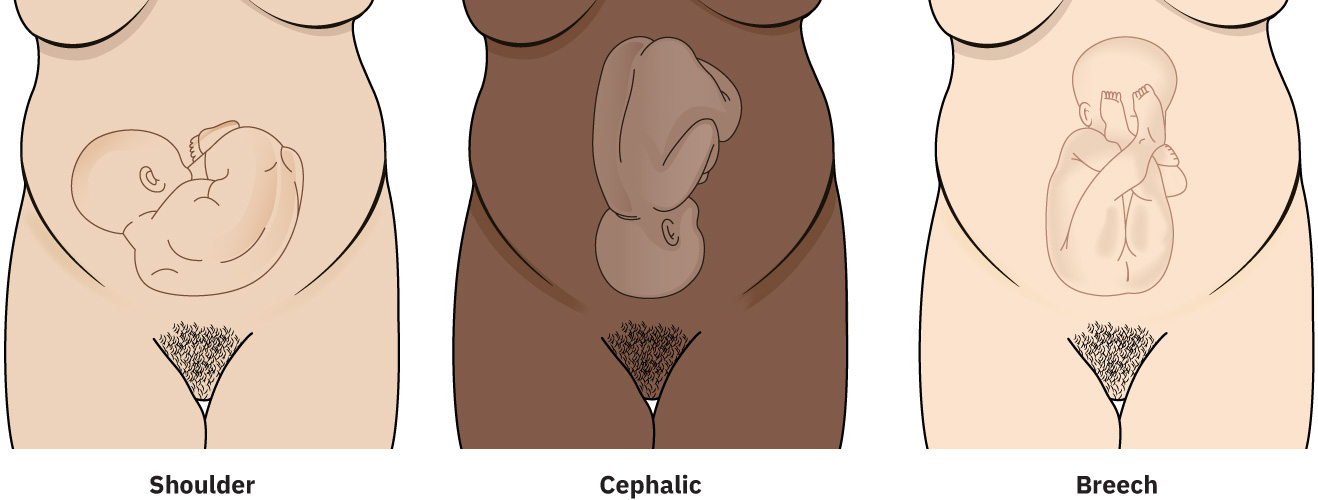 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.4.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.11.4.
- Attitude: Degree of head/neck flexion-extension (for example, vertex, brow, face). Flexed head/neck (vertex) is typical at term because it reduces the presenting diameter; deflexion/extension increases brow or face presentation risk, and face presentation reflects complete extension at the pelvic inlet.
- Position: Relationship of presenting part to maternal pelvis landmarks (for example, LOA, ROA, LOP, ROP, OT, mentum variants).
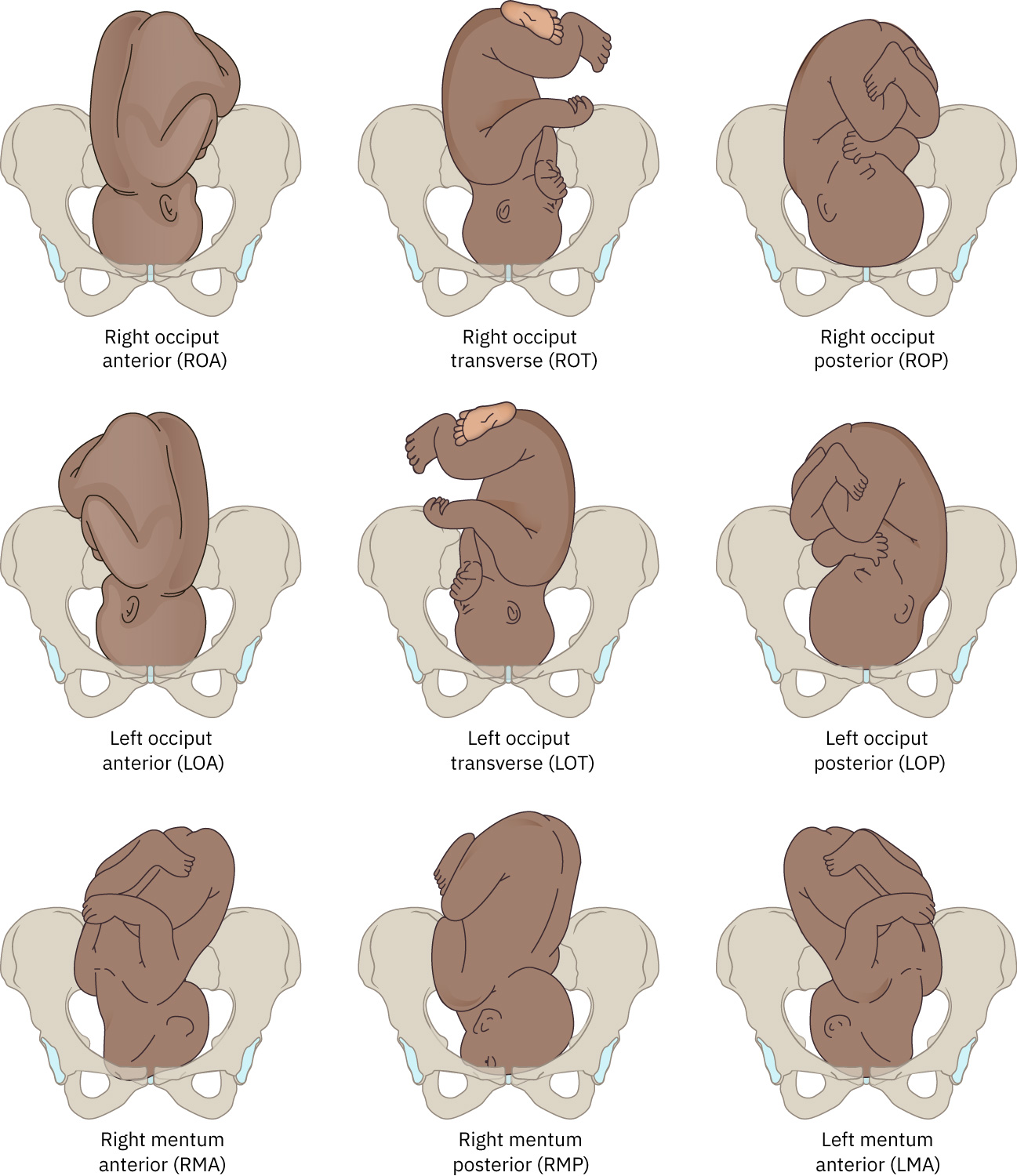 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
- Station: Presenting-part level relative to ischial spines from
-5to+5;0is engagement.
Common malpresentation and malposition risk factors:
- Unstable lie
- Large-for-gestational-age fetus
- Multiple gestation
- Polyhydramnios
- Contracted pelvis
- Pendulous abdomen
- Uterine anomalies or abnormal placental location
- Preterm gestation
- Grand multiparity
- Abdominal wall laxity
- Uterine fibroids
Cephalic presentation means the fetal head is the presenting part at the lower uterus. Breech presentation means buttocks or lower extremities are presenting; common subtype labels include frank, complete, incomplete, and footling breech. Breech-specific context:
- Breech at term is about 3 to 4 percent; incidence is higher in preterm gestation, and many fetuses convert to cephalic by around 34 weeks.
- Footling breech carries the highest prolapsed-cord risk; frank breech carries lower prolapse risk but still requires careful delivery planning.
- Breech birth carries risk of head entrapment and trauma because the after-coming head may not mold effectively.
- Elective cesarean is commonly favored for selected breech contexts (for example large fetus, oligohydramnios, contracted pelvis, or prior cesarean scar) because perinatal outcome risk is higher.
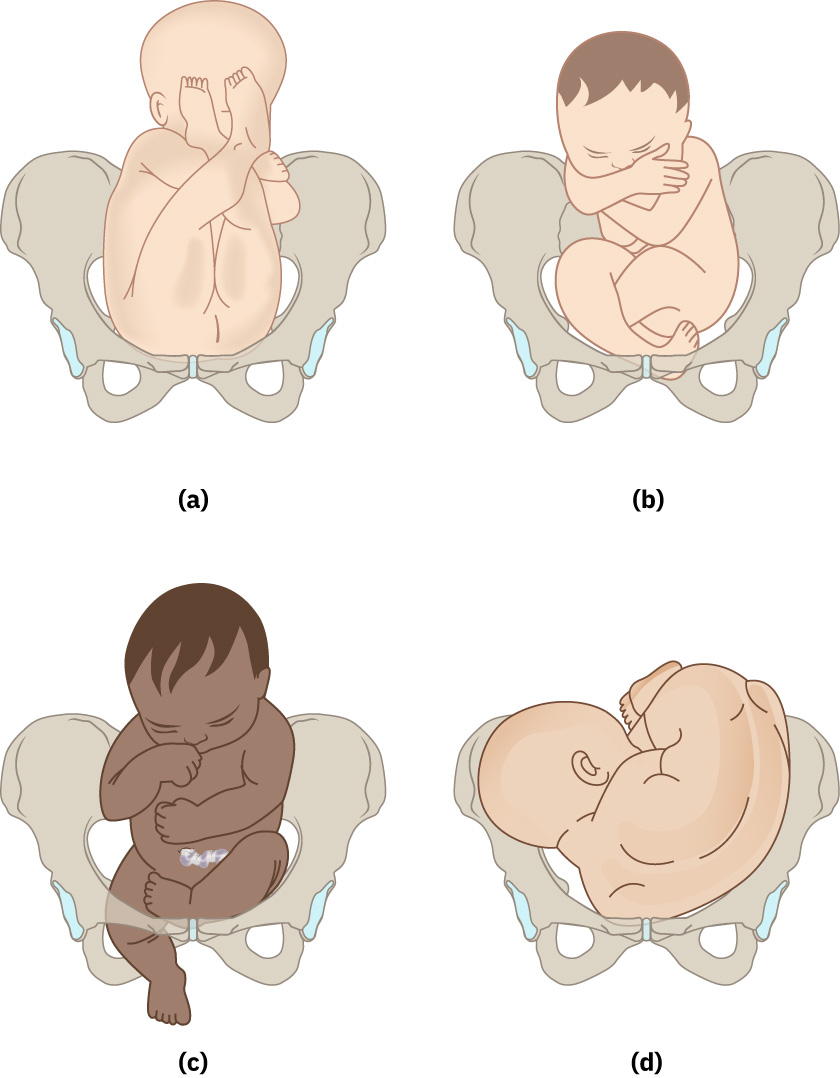 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
Nursing Assessment
NCLEX Focus
Priority questions often test whether fetal alignment explains slow labor progression and which finding requires escalation.
- Use Leopold maneuvers to estimate lie and presenting part before invasive assessment.
- Confirm presenting-part findings with vaginal examination when appropriate and correlate with Leopold results.
- Use a staged workflow: infer likely position from lie/presentation/fetal-back location and attitude on Leopold exam, then map final position to maternal pelvic landmarks from digital exam features of the presenting part.
- During vaginal examination, identify sagittal suture and fontanelle landmarks to infer occiput orientation and fetal attitude.
- For vertex assessment, trace sagittal-suture orientation (anterior-posterior, oblique, or transverse), then distinguish posterior fontanelle (typically compressed, Y-shaped with three sutures) from anterior fontanelle (diamond-shaped with four sutures).
- Assess whether head entry is synclitic versus anterior/posterior asynclitic, because asynclitic patterns can contribute to abnormal labor progression.
- Track station trend with contraction/pushing context rather than using single measurements in isolation.
- Use ischial spines as station landmarks and recognize that markedly prominent/encroaching spines may indicate limited midpelvic capacity.
- Recognize common terms and abbreviations:
R/L: Right or left maternal pelvis.O/M/S: Occiput, mentum, or sacrum leading point.A/P/T: Anterior, posterior, or transverse maternal reference.
- Escalate for persistent non-longitudinal lie, unclear presentation, or discordant exam findings; request ultrasound confirmation when needed.
- Treat persistent transverse lie at term as high-risk for vaginal-birth incompatibility and escalate early for provider-level delivery planning.
- Integrate passageway clues with orientation findings (inlet, midpelvis, and outlet adequacy) when descent stalls despite adequate contractions.
- Use denominators correctly when communicating position: occiput for vertex, sacrum for breech, mentum for face, and acromion for shoulder presentation.
- Leopold maneuvers can detect many malpositions but have limited rule-in precision; if targeted repositioning is not effective, repeat assessment, test alternatives, and use ultrasound confirmation.
Nursing Interventions
- Optimize maternal positioning and mobility to support rotation/descent when safe.
- Match position strategy to descent level: when head is high, favor walking/swaying, birth-ball hip movement, or lunge/side-lying; when head is low but stalled, use supported squatting, upright positions, or hands-and-knees rocking.
- Communicate fetal orientation findings clearly during handoff and provider updates.
- Reinforce patient/family education in plain language on how fetal orientation affects labor progress and intervention options.
- Prepare for operative/cesarean contingency when presentation or lie is incompatible with safe vaginal progression.
- For occiput posterior malposition, support rotation-promoting maternal positions (hands-and-knees, forward-leaning, or side-lying) and reassess descent/rotation trend.
- For face presentation, communicate mentum orientation clearly: mentum-anterior may pass through the outlet, whereas persistent mentum-posterior usually requires cesarean pathway escalation.
- Consider adjunct support such as side-lying release with peanut-ball positioning or rebozo counterpressure techniques when unit expertise and patient preference support use.
- For persistent oblique or transverse lie near term, align counseling with likely ECV candidacy versus cesarean pathway and reinforce that failed correction often leads to planned operative birth.
External Cephalic Version (ECV) Considerations
ECV is a provider-performed abdominal maneuver to rotate a malpresenting fetus into cephalic lie before or during labor-adjacent decision windows.
- Reported ECV success is about 58 percent.
- Higher success contexts include multiparity, unengaged presenting part, posterior placenta, and normal amniotic fluid volume.
- Contraindications include vertical cesarean scar history, multiple gestation, oligohydramnios, uterine/fetal anomalies, nonreassuring FHR, and fetal growth restriction.
- Procedure risk counseling includes transient fetal bradycardia/FHR abnormalities, membrane rupture, vaginal bleeding, cord prolapse, placental abruption, stillbirth, and emergency cesarean birth.
- Uterine-relaxation adjuncts may include terbutaline, nifedipine, or epidural support.
- Fetal status monitoring commonly uses ultrasound and/or Doppler during attempts to elevate the presenting part and rotate toward cephalic lie.
- Manual rotation pathways may move the fetus from breech through transverse orientation into cephalic presentation when successful.
- Nursing role includes consent verification, medication/analgesia preparation per order, continuous fetal assessment, and immediate operating-room/team readiness if deterioration or failed ECV requires urgent cesarean.
- If ECV succeeds, vaginal-birth candidacy may be restored; if unsuccessful, scheduled cesarean planning is typical.
Misclassification Risk
Misidentifying fetal position can delay needed intervention and worsen maternal-fetal outcomes; use repeat assessment and imaging when uncertainty remains.
Clinical Judgment Application
Clinical Scenario
A laboring patient has slow descent despite strong contractions, and exam suggests persistent occiput posterior orientation.
- Recognize Cues: Adequate power with limited descent progression.
- Analyze Cues: Passenger-position factor is likely limiting progress.
- Prioritize Hypotheses: Persistent malposition with rising dystocia risk.
- Generate Solutions: Repositioning strategy, focused reassessment, and provider notification.
- Take Action: Implement position changes and reassess station/rotation trend.
- Evaluate Outcomes: Descent improves, or escalation to procedural delivery planning occurs.
Related Concepts
- factors-influencing-the-process-of-labor-and-birth - Passenger and passageway domains depend on fetal orientation.
- nursing-care-during-the-first-stage-of-labor - Early orientation assessment supports triage and progression interpretation.
- nursing-care-during-the-second-stage-of-labor - Position and station trends guide pushing support and escalation timing.
- labor-dystocia - Malposition and malpresentation are major causes of prolonged labor.
- fhr-and-uc-intervention-framework - Nonreassuring fetal patterns may emerge when descent is obstructed.
Self-Check
- Which lie/presentation combinations are generally compatible with vaginal birth?
- How does station trend refine interpretation of pushing effectiveness?
- Which exam uncertainties should prompt bedside ultrasound confirmation?