FHR and Uterine Contraction Intervention Framework
Key Points
- Nursing response to abnormal tracings is cause-focused, not pattern-label-only.
- Reversible contributors include tachysystole, hypotension, positioning, and medication effects.
- Category III patterns require immediate intrauterine resuscitation and expedited birth planning.
Pathophysiology
Abnormal fetal heart rate (FHR) and uterine contraction (UC) patterns often reflect interrupted oxygen transfer, excessive uterine workload, or transient medication effects. Rapid differentiation between reversible physiologic drivers and escalating pathologic compromise determines outcomes.
Baseline abnormalities (tachycardia, bradycardia), variability changes, and decelerations are interpreted with contraction context and maternal status. Effective nursing care uses a standardized escalation sequence while repeatedly reassessing response after each intervention.
Classification
- Baseline rate concerns: Tachycardia or bradycardia requiring etiology-focused correction.
- Variability concerns: Loss of moderate variability or marked variability patterns requiring targeted investigation.
- Deceleration concerns: Early, late, variable, and prolonged patterns with differing urgency.
- Tiered interpretation: Category I (reassuring), Category II (indeterminate), Category III (abnormal/high-risk).
- Category transition cues: Category II includes mixed intermediate findings; Category III requires absent variability with recurrent late or variable decelerations, bradycardia, or sinusoidal pattern.
- Sinusoidal concern cue: Smooth regular wave-like tracing (about 3 to 5 cycles per minute) with absent true variability warrants urgent evaluation for severe fetal compromise such as anemia/blood-loss contexts.
Nursing Assessment
NCLEX Focus
Priority items test which intervention comes first when fetal compromise signs emerge alongside uterine hyperstimulation or maternal instability.
- Correlate tracing findings with maternal hemodynamics, medications, and contraction burden.
- Separate transient medication-related baseline/variability effects (for example narcotics, magnesium sulfate, terbutaline, or butorphanol exposure context) from persistent pathologic deterioration.
- Interpret minimal variability with differential context (sleep cycle, prematurity, medication exposure, CNS factors) and trend response rather than concluding compromise from one segment alone.
- Treat absent variability or rapid decline from moderate to minimal/absent as urgent deterioration signal requiring immediate escalation workflow.
- For marked variability, increase reassessment frequency and provider communication because baseline interpretation may be unstable during potential hypoxia stress.
- Treat marked variability as uncommon and potentially poststress (for example after seizure or cord-compression events), with rapid reassessment and oxygen/perfusion optimization.
- Distinguish monitoring method limits: external toco best captures frequency/duration trends, while internal pressure catheters provide quantified uterine tone/intensity context.
- When internal monitoring is used, interpret uterine tone/intensity with expected context (resting tone often around 10-12 mmHg; active labor acme commonly higher, and pushing can reach very high pressures).
- When IUPC data are available, calculate Montevideo units from the 10-minute sum of each contraction peak minus resting tone to evaluate contraction adequacy more precisely.
- Check for immediately reversible causes such as prolapsed cord, rapid descent, or tachysystole.
- In recurrent late-deceleration patterns, prioritize uteroplacental-perfusion causes (tachysystole/oxytocin burden, maternal hypotension after neuraxial anesthesia, hypertensive/placental pathology).
- For variable decelerations, prioritize cord-compression differential even when contractions are not temporally aligned, and escalate urgency as repetitive depth/duration burden increases.
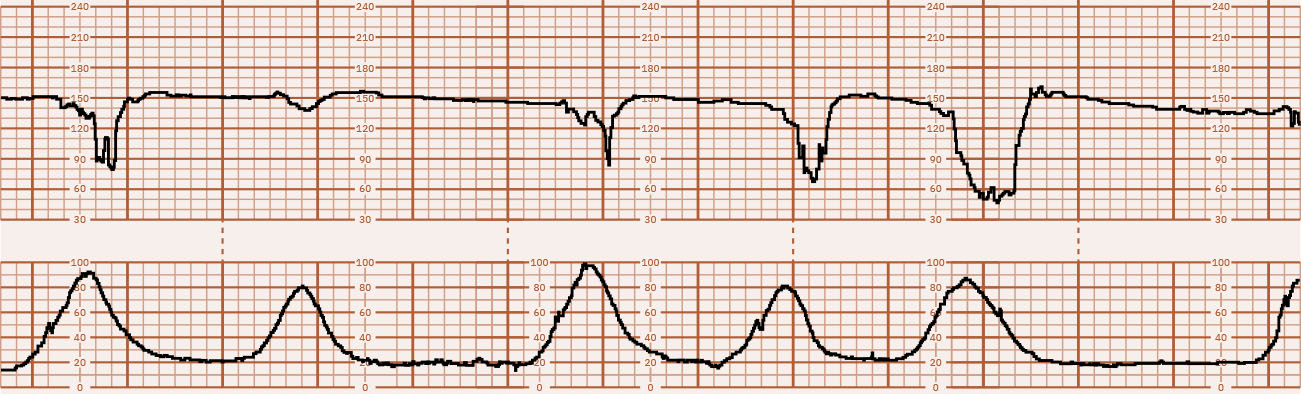 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
- For prolonged decelerations, investigate uterine hyperactivity, cord compression, maternal hypotension, placental abruption, seizure activity, and imminent birth context.
- When baseline rate falls, distinguish true sustained bradycardia from prolonged deceleration pattern before final classification.
- Determine category trend (I, II, III) and whether current findings are improving or worsening.
- For Category II tracings, evaluate specifically for accelerations and moderate variability; when both are not present, begin intrauterine resuscitation while reassessment continues.
- Use gestational-age appropriate acceleration criteria when interpreting reassurance (10x10 before 32 weeks; 15x15 at/after 32 weeks).
- Use standardized charting sequence: monitoring method (external/internal), baseline rate and variability, accelerations/decelerations with type, contraction pattern (frequency-duration-intensity and resting tone if internal), category, and plan of care/communications.
- During oxytocin titration, chart fetal status before and after each rate increase.
- Reassess frequently after each intervention rather than waiting for prolonged deterioration.
- After a prolonged deceleration resolves, reassess immediately for residual tachycardia or worsening variability that may indicate significant hypoxic burden.
- For fetal tachycardia, prioritize maternal fever assessment (notably 38 C or higher), then hydration, anemia, thyroid history, and infection/hypoxia contributors.
- Match action level to category: Category I usually routine surveillance, Category II continued surveillance with repeated reassessment and timely provider updates, Category III immediate provider contact with resuscitation and expedited-birth planning if unresolved.
Nursing Interventions
- For tachysystole with nonreassuring FHR, discontinue oxytocin immediately, reposition laterally, provide IV bolus support (commonly 500 mL LR if not contraindicated), apply oxygen 8-10 L/min by mask, and prepare/administer terbutaline per order.
- For tachysystole with reassuring FHR, reposition laterally and provide IV bolus; if unresolved after about 10 minutes reduce oxytocin by half, and if still unresolved after another 10 minutes discontinue oxytocin until contraction frequency normalizes (5 or fewer in 10 minutes).
- If terbutaline is considered, verify maternal pulse before administration and generally hold when pulse is above 120 bpm; anticipate transient maternal/fetal heart-rate increase after dosing.
- For fetal bradycardia concern, execute immediate first-line sequence (reposition, IV fluid bolus when indicated, prompt provider notification) while tracing trend is reassessed continuously.
- If bradycardia occurs during oxytocin use, discontinue oxytocin immediately before additional steps; if not on oxytocin, begin repositioning first.
- Perform prompt cervical exam for bradycardia/prolonged deceleration to assess cord prolapse or rapid fetal descent.
- If cord prolapse is identified, manually elevate presenting part off the cord and maintain decompression continuously while emergent cesarean birth is prepared.
- For fetal tachycardia with maternal fever, notify provider for antipyretic/anti-infective management and support hydration/perfusion.
- Use conservative intrauterine resuscitation first for variable decelerations and avoid additional sedating analgesia when fetal status is nonreassuring until provider reassessment.
- Perform focused vaginal exam when clinically indicated to identify urgent mechanical causes.
- Assist with amnioinfusion when prescribed for recurrent variable decelerations with cord-compression concern, and monitor uterine pressure to avoid overdistention.
- Notify provider early with precise tracing description and intervention-response timeline.
- Early deceleration patterns usually require labor-progress assessment and birth readiness rather than aggressive resuscitation unless additional abnormal features develop.
Nonresponse Escalation
Category II patterns that do not improve with intrauterine resuscitation can progress to Category III and require urgent delivery planning.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| uterotonics | Oxytocin context | Stop or adjust promptly when contraction excess contributes to fetal compromise. |
| tocolytics | Terbutaline context | Consider for tachysystole or elevated resting tone when ordered. |
Clinical Judgment Application
Clinical Scenario
A laboring patient on oxytocin develops recurrent variable decelerations, then persistent late decelerations with minimal variability.
- Recognize Cues: Worsening periodic changes and variability decline with ongoing contraction stress.
- Analyze Cues: Fetal oxygen reserve may be depleting with possible uteroplacental compromise.
- Prioritize Hypotheses: Most urgent issue is evolving hypoxia requiring immediate corrective bundle.
- Generate Solutions: Stop oxytocin, lateral repositioning, fluid support, evaluate for tachysystole/mechanical causes, notify provider.
- Take Action: Execute interventions in sequence and document response timing.
- Evaluate Outcomes: Improvement in tracing stabilizes care; persistent deterioration triggers expedited birth pathway.
Related Concepts
- fetal-heart-rate-and-contraction-patterns - Terminology foundation for interpretation.
- physiological-influences-on-fetal-heart-rate-patterns - Etiology guides intervention choice.
- external-and-internal-fetal-monitoring - Data quality affects confidence in intervention decisions.
- intrauterine-resuscitation - Core intervention set for nonreassuring fetal status.
- oxytocin-therapy - Uterotonic management is tightly linked to contraction-related fetal risk.
Self-Check
- Which immediate interventions are prioritized for bradycardia with tachysystole?
- How does management differ between resolving Category II and persistent Category III tracings?
- Why is intervention-response timing documentation clinically critical?