Nursing Care during the Second Stage of Labor
Key Points
- Second-stage care prioritizes coordinated pushing support, fetal surveillance, and maternal safety.
- Maternal assessments include frequent vital signs, contraction trend, descent progress, and fatigue.
- Fetal heart rate monitoring must rapidly identify compromise and trigger escalation.
Pathophysiology
The second stage begins at complete cervical dilation (10 cm with complete effacement) and ends with birth of the newborn. During this stage, uterine contractions and maternal bearing-down efforts combine to move the fetus through the pelvis while fetal oxygen reserve is repeatedly challenged by contraction stress.
Nursing support influences both physiologic efficiency and safety. Position changes, breathing guidance, and targeted coaching can optimize descent mechanics and reduce unnecessary maternal exhaustion while preserving fetal tolerance.
Classification
- Maternal-support domain: Positioning, rest-push balance, comfort measures, and emotional coaching.
- Fetal-monitoring domain: Continuous or intermittent surveillance for distress patterns.
- Preparation domain: Delivery setup, newborn warmer readiness, and team coordination.
- Complication domain: Slow descent, excessive bleeding, shoulder dystocia risk, and maternal fatigue.
- Cardinal-movement domain: Engagement, descent/rotation, extension, restitution, and shoulder delivery sequence.
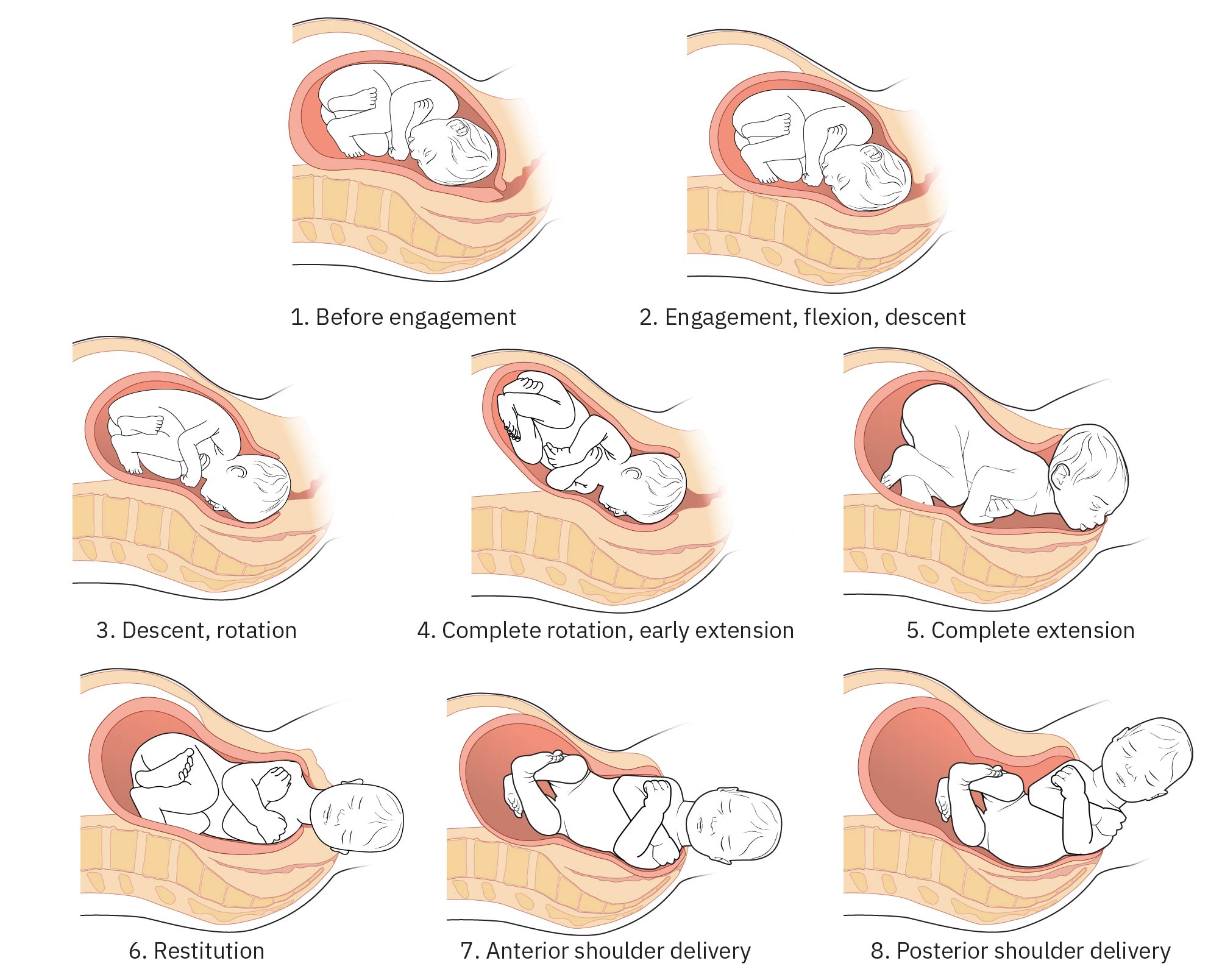 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.2.
Nursing Assessment
NCLEX Focus
Priority questions ask which finding in second stage requires immediate provider notification and which support action should be implemented first.
- Monitor maternal vital signs at least every 30 minutes and contraction pattern about every 15 minutes.
- Trend temperature by membrane and risk status (for example every 4 hours with intact membranes, every hour after membrane rupture, and every hour in febrile/high-risk contexts).
- Distinguish expected pushing-related tachycardia from sustained maternal heart rate escalation (for example persistent above 120 bpm), and pair reassessment with temperature/fetal status to screen for emerging infection complexity.
- Assess pushing effectiveness, energy conservation, and signs of physical or emotional exhaustion.
- Track fetal station progression, crowning, and fetal heart rate response to contractions and pushing.
- In second stage, reassess fetal heart baseline/variability/periodic changes at least every 5 to 15 minutes and escalate immediately for nonreassuring shifts.
- Use noninvasive progress cues (perineal bulging, visible presenting part, maternal stool passage) to limit unnecessary repeated vaginal examinations when possible.
- Use parity and epidural context for expected duration ranges (for example nulliparous about 2 to 3 hours without epidural or 3 to 4 hours with epidural; multiparous about 1 hour or up to 2 hours with epidural).
- Evaluate for failure to descend when fetal station does not change for 2 hours despite sustained pushing effort.
- Identify complication cues such as abnormal fetal tracing, prolonged second stage, excessive bleeding, or dystocia concern.
- During fetal-distress concern, include amniotic-fluid reassessment (color, odor, and meconium status) alongside maternal-vital and tracing review.
- Use parity and epidural context when evaluating second-stage duration expectations and need for escalation.
- For prolonged pushing trajectories (for example exceeding about 3 hours multiparous or 4 hours nulliparous), review rising maternal-fetal risk profile and escalate shared decision-making with provider and patient.
- Monitor intake and output continuously during active pushing to detect dehydration, bladder distention, or perfusion-related concerns.
Nursing Interventions
- Coach pushing with stage-appropriate breathing and individualized strategy (open or closed glottis).
- Explain that open- and closed-glottis pushing are both effective in current evidence and support patient preference when maternal-fetal status remains reassuring.
- When maternal-fetal status is reassuring, align pushing onset with patient urge (immediate or delayed) and support spontaneous pushing when effective progress is present.
- If maternal status acutely worsens (for example sustained tachycardia with fever), perform rapid full reassessment, notify provider, and adapt pushing plan based on updated maternal-fetal safety priorities.
- If progress is unclear early in second stage, modify pushing strategy and position within the first 30 minutes (for example redirect bearing-down, switch open/closed glottis coaching, or change posture).
- Promote position changes that support descent and comfort while maintaining monitoring quality.
- Favor upright or side-lying positions over prolonged lithotomy/supine positioning when feasible because outcomes for descent, pain, and fetal tolerance are often improved.
- Apply comfort measures such as warm compresses, massage, and cool-cloth support.
- Consider perineal massage support in second stage to reduce episiotomy likelihood in selected patients.
- Support hydration and calorie replenishment during prolonged labor and consider laboring down before renewed active pushing when clinically appropriate.
- Offer sips of water or ice chips when clinically appropriate to support hydration and coping.
- Maintain continuous bedside presence during active pushing while preparing sterile birth field and newborn resuscitation readiness.
- Prepare delivery-table and infant-warmer readiness (including oxygen/suction functionality and preheating) before birth.
- Verify newborn-warmer checklist readiness before delivery (for example bag-mask device, suction setup, oxygen source/tubing, airway tools, thermoregulation supplies, pulse oximetry, cord clamps/scissors, Apgar timing tools, and emergency-medication access per policy).
- Brief the birthing person and family on expected bedside team members and roles before birth to reduce overwhelm during immediate newborn transition.
- Assign dedicated newborn support at delivery (for example an additional nurse for newborn assessment and initial resuscitation steps) and include respiratory/support staff per facility policy.
- Maintain frequent, structured communication with the provider on fetal heart trends, descent progress, pushing effectiveness, and any maternal-status changes.
- Perform perineal hygiene with warm water or moist cloths and cleanse front to back according to policy to reduce contamination during second-stage care.
- Anticipate the cardinal mechanisms of birth near crowning and escalate promptly for nonprogressive descent or shoulder dystocia cues.
- During head delivery, anticipate restitution and subsequent external rotation; recognize incomplete shoulder restitution or impaction as potential shoulder-dystocia warning.
- If shoulder dystocia occurs, assist immediate maneuver sequence (McRoberts position, suprapubic pressure, and provider-directed repositioning such as hands-and-knees) while documenting timing and responses.
- For precipitous/rapid delivery with delayed provider arrival, support controlled head/shoulder delivery and immediate newborn safety steps per policy.
- Use a shared decision framework when discussing prolonged second-stage management options, including continued pushing versus operative vaginal pathway versus cesarean escalation.
Fetal Distress and Dystocia Risk
Abnormal fetal heart patterns or signs of shoulder dystocia require immediate escalation and coordinated emergency response.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| labor-analgesics | Epidural and non-epidural options | Analgesia choice affects pushing sensation, coaching strategy, and movement support. |
| uterotonics | Oxytocin labor context | Contraction pattern and fetal response must be monitored closely during use. |
Clinical Judgment Application
Clinical Scenario
A patient with complete dilation has prolonged pushing, rising fatigue, and intermittent nonreassuring fetal heart changes.
- Recognize Cues: Decreasing push effectiveness, slower descent, and fetal stress indicators.
- Analyze Cues: Maternal exhaustion and contraction stress may be reducing safe progression.
- Prioritize Hypotheses: Immediate priority is fetal safety while restoring effective maternal effort.
- Generate Solutions: Adjust position, refine coaching, optimize rest between contractions, and update provider.
- Take Action: Implement support bundle and increase surveillance frequency.
- Evaluate Outcomes: Descent progresses and tracing stabilizes, or expedited operative plan is activated.
Related Concepts
- stages-of-labor - Defines transition points and expected second-stage progression.
- fetal-heart-rate-and-contraction-patterns - Pattern interpretation directs urgent decisions.
- nonpharmacological-pain-management - Comfort strategies improve coping and pushing efficiency.
- intrauterine-resuscitation - Needed when second-stage fetal oxygenation becomes compromised.
- labor-dystocia - Slow progression framework informs escalation thresholds.
Self-Check
- Which second-stage findings indicate progression versus arrest of labor?
- How do open and closed glottis pushing strategies influence coaching?
- Which cues require immediate escalation for possible shoulder dystocia or fetal compromise?