Benign Prostatic Hyperplasia
Key Points
- BPH is the most common prostate disorder — affects >50% of men aged 51–60 years and ~70% of men older than 60 years; benign, age-related prostate enlargement.
- Mechanism: Enlarged prostate presses against the urethra → lower urinary tract symptoms (LUTS): urinary hesitancy, weak stream, frequency, nocturia, incomplete emptying.
- Diagnostics: Symptom scoring plus PSA, DRE, and selected urologic studies (urodynamic flow testing, voiding cystourethrogram, cystoscopy).
- Pharmacotherapy: α₁-adrenergic antagonists (tamsulosin, terazosin) relax smooth muscle → improve flow; 5-α-reductase inhibitors (finasteride) reduce prostate size.
- Surgical: TURP (transurethral resection of the prostate) — most common; post-op nursing priority is continuous bladder irrigation (CBI) monitoring.
- Key nursing concern: α₁-blockers cause orthostatic hypotension — educate patient to rise slowly.
Pathophysiology
The prostate gland is located directly below the urinary bladder surrounding the proximal urethra. With aging, the gland undergoes benign enlargement (hyperplasia). As the prostate grows larger, it compresses the urethra, obstructing urinary outflow and causing:
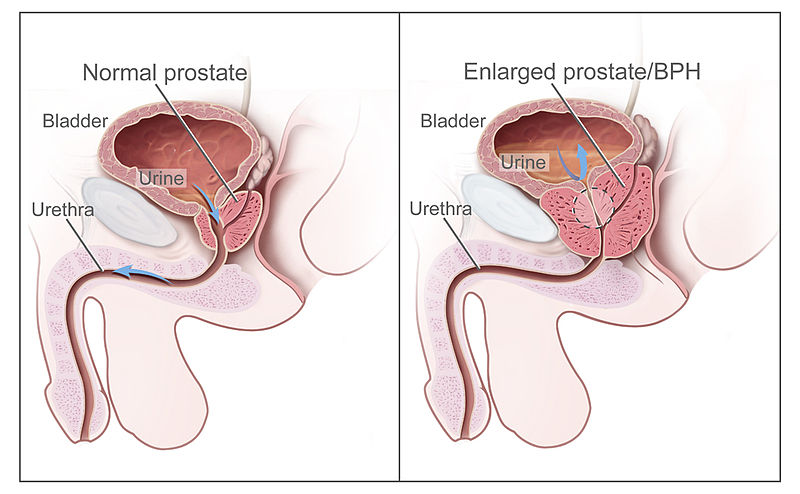 Illustration reference: OpenRN Nursing Health Promotion Ch.8.9.
Illustration reference: OpenRN Nursing Health Promotion Ch.8.9.
- Incomplete bladder emptying
- Bladder overdistension and detrusor muscle dysfunction
- Increased risk of UTI, urinary retention, and hydronephrosis if untreated
BPH is not cancerous — it does not increase risk of prostate cancer; however, BPH and prostate cancer may coexist in the same patient.
Clinical Manifestations (LUTS)
| Symptom | Description |
|---|---|
| Urinary hesitancy | Difficulty initiating urinary stream |
| Weak or intermittent stream | Starts and stops; dribbling at end of stream |
| Nocturia | Frequent nighttime urination |
| Urinary frequency | Increased voiding, often small amounts |
| Incomplete emptying | Feeling of residual urine after voiding |
| Urinary urgency | Sudden strong urge to void |
| Recurrent UTI/kidney stones | From urinary stasis and retention |
| Hematuria | Late sign of prostate-cancer (prostate cancer) (not typical of BPH alone) |
Assessment and Diagnostics
- Digital Rectal Examination (DRE): Provider inserts lubricated finger into rectum to assess prostate size and texture
- BPH: smooth, uniformly enlarged prostate
- Prostate cancer: hard nodule on prostate
- PSA (Prostate-Specific Antigen): Blood test — elevated with BPH or prostate cancer; screening guidelines: test every 2 years if PSA <2.5 ng/mL; annually if PSA >2.5 ng/mL
- International Prostate Symptom Score (I-PSS): Standardized questionnaire assessing LUTS severity
- Urinalysis: Screens for UTI, hematuria, kidney stones (common complications of BPH)
- Post-void residual (PVR) measurement: Determines amount of urine remaining after voiding (>100 mL indicates significant retention)
- Urodynamic flow testing: Assesses bladder/sphincter/urethral storage and release performance, including involuntary contraction patterns
- Voiding cystourethrogram (VCUG): Fluoroscopy with contrast during filling and voiding to evaluate urinary-tract anatomy and urine-flow direction
- Cystoscopy: Direct urologic visualization of urethral/prostatic obstruction
Pharmacological Treatment
| Drug Class | Examples | Mechanism | Key Adverse Effects |
|---|---|---|---|
| α₁-Adrenergic antagonists | Tamsulosin, Terazosin, Doxazosin, Alfuzosin | Relax smooth muscle in bladder neck and prostate → improved urine flow | orthostatic-hypotension (Orthostatic hypotension), dizziness, headache, syncope |
| 5-alpha-reductase-inhibitors | Finasteride, Dutasteride | Block conversion of testosterone to dihydrotestosterone (DHT) → reduces prostate size over months; maximal response often around 6 months with PSA decline of about 50% | Decreased libido, erectile-dysfunction (erectile dysfunction), decreased ejaculatory volume, gynecomastia |
| Combination and adjunct therapy | Finasteride + doxazosin, dutasteride + tamsulosin, alpha-blocker + antimuscarinic | Improves symptom burden/flow in selected clients; antimuscarinics may be used for overactive bladder symptoms | Monitor orthostasis, anticholinergic burden, and urinary retention risk |
| PDE-5 inhibitors | Tadalafil (Cialis) | Relax smooth muscle in urinary tract; FDA-approved for BPH symptoms | Facial flushing, headache, diarrhea; contraindicated with nitrates |
Orthostatic Hypotension
Alpha-1 blockers (tamsulosin, terazosin) cause orthostatic hypotension — especially with first dose. Educate patient to rise slowly from sitting/lying; fall precautions for older adults.
Surgical Interventions
| Procedure | Description | Post-Op Care |
|---|---|---|
| TURP (most common) | Resectoscope via urethra; trims prostate tissue; continuous bladder irrigation (CBI) after | Monitor CBI patency; urine color (pink-tinged with no clots = good); catheter care |
| TUNA | Radiofrequency needles via urethra destroy excess prostate tissue | Monitor urinary output |
| TUMT | Microwave antenna via urethra destroys excess tissue | — |
| PVP (GreenLight photovaporization) | Laser energy vaporizes excess prostate tissue | Monitor post-procedural urinary flow and bleeding cues |
| Additional transurethral thermal techniques | High-intensity focused ultrasound, transurethral electrovaporization, water-induced thermotherapy | Used when medication response is limited; monitor urinary flow/retention changes |
| Prostatic stent | Spring-like stent widens narrowed urethral segment | Option for selected nonsurgical pathways; monitor discomfort, obstruction, and infection signs |
| TUIP / Laser surgery | Urethral/bladder neck incisions or laser tissue ablation via cystoscope | Lower-pressure outlet strategy with bleeding-risk surveillance |
| UroLift | Permanent implants hold back enlarged tissue — less invasive | — |
| Simple prostatectomy | Remove excess prostate tissue via abdominal/perineal incision; most invasive | 2–4 day hospital stay |
Post-TURP Nursing Priorities
- Continuous Bladder Irrigation (CBI): Three-way Foley catheter irrigates bladder to prevent clot formation and obstruction
- Adjust irrigation flow to maintain patent drainage
- Expected: pink-tinged urine with few or no clots = adequate irrigation
- Bright red urine or large clots → notify provider; possible arterial bleeding
- Calculate true urine output by subtracting irrigation volume instilled from total drainage output
- Use a large drainage bag to accommodate high irrigant-return volumes
- Catheter care: Prevent catheter-associated UTI with meticulous technique
- Complication surveillance: Track painful bladder spasms, clot retention, persistent heavy hematuria, DVT cues (calf pain/unilateral warmth-swelling), infection signs, and delayed voiding recovery
- Psychosocial support: Urinary and sexual symptoms are personal; postoperative incontinence or sexual dysfunction may be temporary but distressing
Nursing Interventions
- Assess voiding pattern and PVR residual
- Educate on fluid timing (especially before bedtime), caffeine/alcohol reduction, and bladder-retraining strategies including double voiding and pelvic floor work
- For nutrition counseling, reinforce Mediterranean-style meal patterns (plant-forward intake and healthier fat substitution) as an adjunct to reduce LUTS burden.
- Voiding schedule: void every 2 hours to prevent over-distension
- Review symptom-worsening medication triggers (for example decongestants, antihistamines, some antidepressants, and diuretics) with prescriber-guided adjustment
- Medication education: alpha-blockers → rise slowly; 5-alpha-reductase inhibitors → delayed onset; report adverse effects and persistent urinary symptoms
- Reinforce tablet-handling safety for 5-alpha-reductase inhibitors: pregnant individuals or those who may become pregnant should avoid contact with crushed or broken tablets.
- Post-procedure: meticulous catheter care, CBI monitoring with accurate output accounting, and escalation of bleeding/clot burden or infection signs
- If urinary-pattern improvement is not achieved after therapy, escalate for treatment-plan revision and additional diagnostics.
- Include psychosocial follow-up and counseling-resource referral when urinary/sexual symptom burden is affecting quality of life.
Related Concepts
- erectile-dysfunction — 5-α-reductase inhibitors (finasteride) and alpha-blockers may cause or worsen erectile dysfunction.
- urinary-system — Prostate anatomy and relationship to urinary outflow obstruction.
- alpha-blockers — Alpha-1 antagonists are first-line pharmacotherapy for BPH symptoms.
- postvoid-residual-measurement-and-retention-management — PVR measurement is essential in BPH to quantify urinary retention.
- kidney-disease — Severe untreated BPH can cause hydronephrosis and progress to CKD.
Self-Check
- A patient newly prescribed tamsulosin for BPH calls to report dizziness when standing. What is the priority nursing response?
- Following TURP, the nurse notes the patient’s continuous bladder irrigation drainage is dark red with visible clots. What is the priority action?
- Why would a patient with BPH be at increased risk for urinary tract infections?