Peritoneal and Hemodialysis Nursing Management
Key Points
- Dialysis is used when kidneys cannot adequately clear fluid, electrolytes, and waste.
- Peritoneal dialysis uses the peritoneal cavity as the exchange membrane, with CAPD (manual daytime exchanges) or CCPD (automated nighttime cycling).
- Hemodialysis uses an external filter and vascular access in clinic or hospital settings, commonly three- to four-hour sessions several times weekly.
- Both PD and HD rely on osmosis and solute diffusion between blood and another compartment.
- CRRT is continuous (often 24 hours/day) and is used when slower fluid/solute removal is needed in hemodynamic instability.
- Emergency HD can begin through a temporary central venous dialysis catheter, while permanent AV fistula access typically requires months to mature.
- Nursing priorities include access-site safety, fluid-electrolyte monitoring, and patient-centered education.
- PD often supports home-based treatment, so nursing teaching on catheter-site care and effluent monitoring is essential.
Pathophysiology
Dialysis supports homeostasis by moving water and solutes across a semipermeable interface through diffusion and osmosis. In peritoneal dialysis (PD), prescribed dialysate is instilled into the peritoneal cavity, dwells to allow exchange with peritoneal capillary blood, and is then drained. In hemodialysis (HD), blood is circulated through an extracorporeal filter and then returned to the patient.
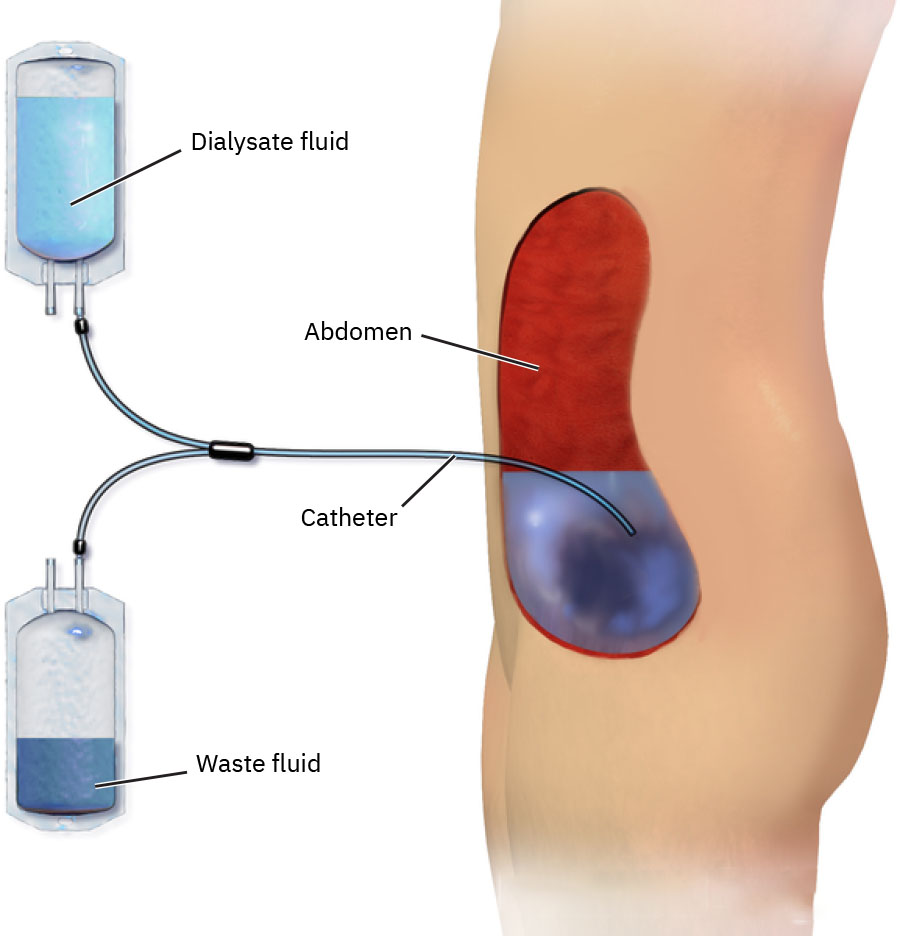 Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
Rapid shifts in fluid and solute balance can improve overload states but also create post-treatment instability, so close monitoring before and after treatment is essential.
Classification
- Peritoneal dialysis: Home-capable modality using intraperitoneal dialysate exchanges via abdominal catheter.
- CAPD: Manual exchanges multiple times per day.
- CCPD: Automated machine-driven exchanges overnight.
- Hemodialysis: Facility-based modality using central catheter or AV access.
- HD catheter types: Nontunneled large-bore central catheter (short-term) and tunneled catheter (permacath) with lower infection risk than nontunneled placement.
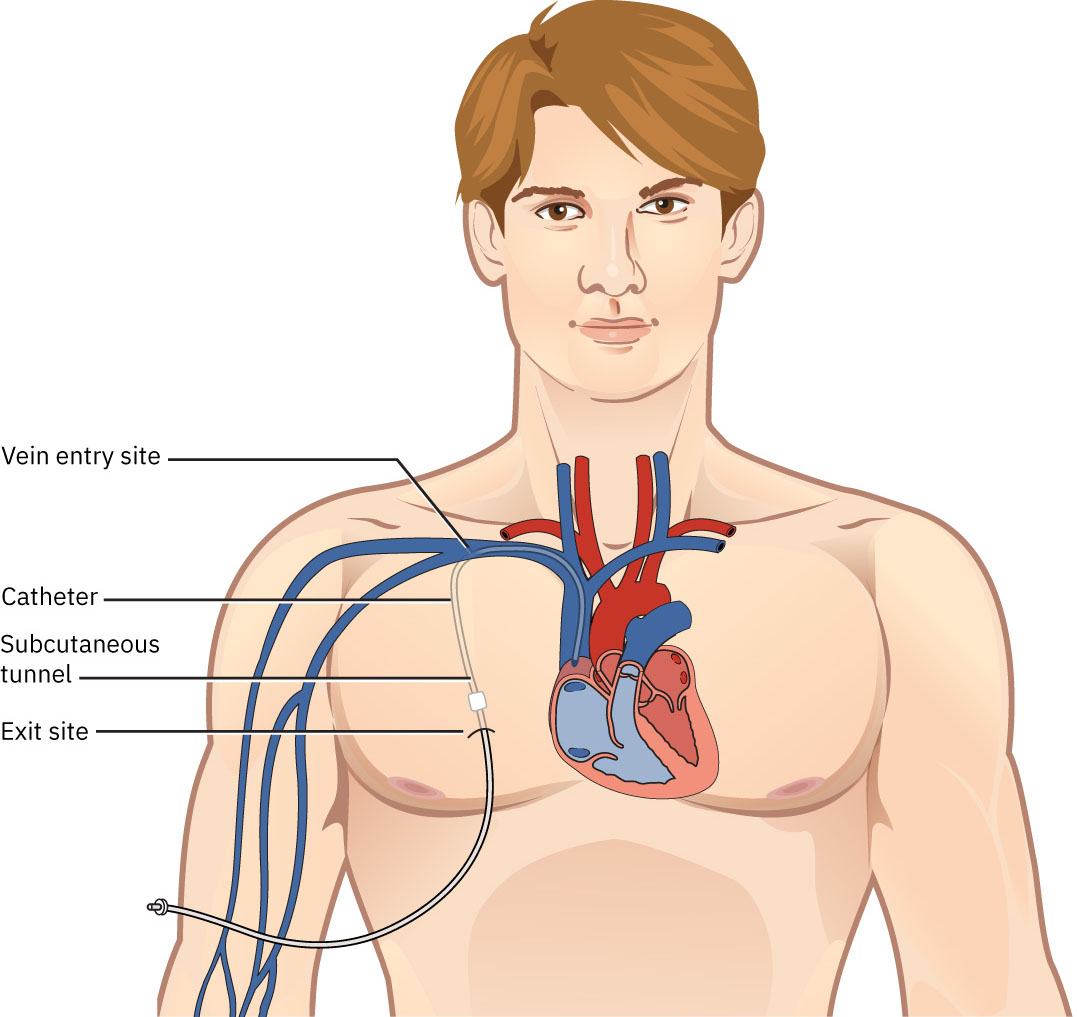 Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
Illustration reference: OpenStax Clinical Nursing Skills Ch.19.4.
- CRRT: Continuous dialysis pathway for unstable ICU-level clients.
- Access-focused care: Infection prevention, patency checks, and dressing integrity.
- Shift-related complication care: Monitoring for pre- and post-dialysis hemodynamic and symptom changes.
Nursing Assessment
NCLEX Focus
Priority is early recognition of access complications and unsafe fluid or electrolyte shifts.
- Assess dialysis access for redness, drainage, tenderness, dressing integrity, and signs of occlusion.
- Confirm expected access pathway for modality (AV fistula/graft or central venous catheter for HD; abdominal catheter for PD).
- For urgent dialysis starts, verify temporary HD catheter status and monitor for central-line complications until long-term access is ready.
- For newly created AV fistula/graft access, assess postsurgical incision healing and early complication cues.
- For AV fistula/graft, assess patency by checking for thrill and bruit at each focused access check.
- Escalate immediately when thrill or bruit is absent because access occlusion may be present.
- Assess volume status trends (weight, edema, dyspnea, blood pressure) around treatment windows.
- Assess for post-treatment symptoms such as hypotension, cramping, nausea, headache, and fatigue.
- During and after dialysis, monitor for dysrhythmia risk from electrolyte shifts and apply continuous telemetry monitoring when ordered.
- Anticipate reduced urine frequency/volume in advanced dialysis-dependent kidney failure and trend change from patient baseline.
- For PD, assess dialysate appearance; expected effluent is typically straw colored.
- For PD, compare instilled dialysate volume with returned effluent, monitor for persistent low return, and assess for leakage around the catheter.
- If PD return is unexpectedly low, assist with repositioning and escalate urgently for possible catheter clogging or dislodgement.
- Assess understanding of access care, fluid limits, and between-treatment self-management.
- For HD central catheters, assess for fever or white-blood-cell rise, and verify dressing remains clean, dry, intact, and occlusive.
Nursing Interventions
- Use strict aseptic technique and protocol-driven access care to reduce infection risk.
- Clean PD catheter insertion site with soap and water or approved antiseptic and keep sterile dressing coverage when not actively connected.
- Coordinate pre-dialysis medication review and hold dialyzable or hypotension-provoking medications as ordered.
- Coordinate pre-dialysis and post-dialysis assessments with closed-loop handoff communication.
- Give complete handoff to the HD nurse during transfer, including patient preferences plus pain, meal, and snack considerations.
- Reinforce individualized fluid and electrolyte guidance between dialysis sessions.
- Teach PD home-care patients when to contact nephrology urgently (no or poor effluent return after repositioning, increasing leakage, cloudy effluent, or access-site infection signs).
- Protect AV fistula/graft as dialysis-only access and monitor for access complications.
- Reinforce that AV fistula access may require a maturation period of several months, so temporary catheter care is often needed during transition.
- Do not use the AV fistula/graft extremity for blood pressure cuffs, venipuncture, or blood draws that can reduce access flow.
- Teach patients to avoid tight clothing and heavy carrying (for example purse or grocery bags) on the affected arm.
- In inpatient settings, use protocol alerts so no blood pressure, IV infusion, blood draw, or tourniquet is applied on the access arm.
- Do not flush AV fistulas between dialysis sessions; preserve site integrity through dialysis-team protocols and routine hygiene teaching.
- If an HD catheter dressing is nonocclusive or drainage is present, perform sterile central-line dressing change per protocol.
- Monitor for HD access complications including infection, sepsis, air embolism (catheter pathway), and fistula/graft occlusion.
- Monitor expected pre-/post-HD physiologic shifts: pre-HD overload or hypertension risk, then post-HD hypovolemia/hypotension risk with nausea, vomiting, headache, cramping, and fatigue; prioritize recovery rest after treatment.
- After return from dialysis, continue high-acuity reassessment on the primary unit because delayed hypotension or rhythm instability may emerge outside the dialysis suite.
- Teach patients that lower urine output after dialysis initiation can be expected while still reinforcing urgent reporting of new pain, fever, or abrupt urinary-pattern change.
- Escalate signs of sepsis, access failure, respiratory compromise, or severe hypotension immediately.
Access and Shift Risk
Dialysis safety depends on both access integrity and vigilant monitoring for rapid hemodynamic or electrolyte change.
Related Concepts
- fluid-volume-overload-hypervolemia - Common pre-dialysis burden requiring surveillance.
- fluid-volume-deficit-hypovolemia-and-dehydration - Possible post-dialysis complication pattern.
- urinary-system - Underlying renal failure context for dialysis dependence.
- postvoid-residual-measurement-and-retention-management - Elimination assessment overlap in renal-urinary care.