Fracture
Key Points
- A fracture is disruption of normal bone integrity and can range from small cracks to complete separation.
- Fracture pattern (for example open, comminuted, or pathologic) affects urgency, infection risk, and treatment pathway.
- Accurate type recognition supports safe reduction, immobilization, and complication surveillance.
- Healing progresses through hematoma, granulation tissue, callus, osteoblastic bone formation, and remodeling phases.
- Global burden is high, with very large annual incidence and ongoing symptom prevalence.
Pathophysiology
Fracture occurs when applied force or underlying bone weakness exceeds structural tolerance. Injury may result from direct trauma, twisting/compression forces, repetitive stress, or disease states that weaken bone.
Clinical severity depends on displacement, skin disruption, number of fragments, and involvement of surrounding soft tissues and neurovascular structures.
Common fracture mechanisms include motor-vehicle collisions, sports injuries, and falls. Surrounding soft tissues are frequently affected, with edema, hemorrhage, tendon injury, and nerve injury often coexisting at the trauma site.
Bone healing begins immediately after injury with hematoma development and proceeds through granulation tissue formation, callus stabilization, osteoblastic woven-bone replacement, and remodeling into stronger lamellar bone. Healing commonly takes about 6 weeks but may extend to months with advanced age, comorbidity, or complication burden.
Classification
- Closed (simple): Bone break without skin penetration.
- Open (compound): Bone break with skin penetration and higher contamination/infection risk.
- Transverse: Fracture line runs straight across the bone.
- Spiral: Twisting force creates a spiral fracture line.
- Comminuted: Bone is broken into multiple fragments.
- Impacted: One bone fragment is driven into another.
- Greenstick: Partial fracture, more common in pediatric clients.
- Oblique: Fracture line crosses bone at an angle.
- Stress fracture: Small crack from repetitive loading.
- Complete fracture: Bone separates fully into two or more pieces.
- Incomplete fracture: Crack without full separation.
- Compression fracture: Bone collapse/crushing pattern, often vertebral.
- Pathologic fracture: Fracture caused by underlying disease-weakened bone.
- Hip-fracture patterns:
- Intracapsular: Femoral-neck fracture within the joint capsule.
- Extracapsular: Fracture outside the capsule involving proximal femur regions.
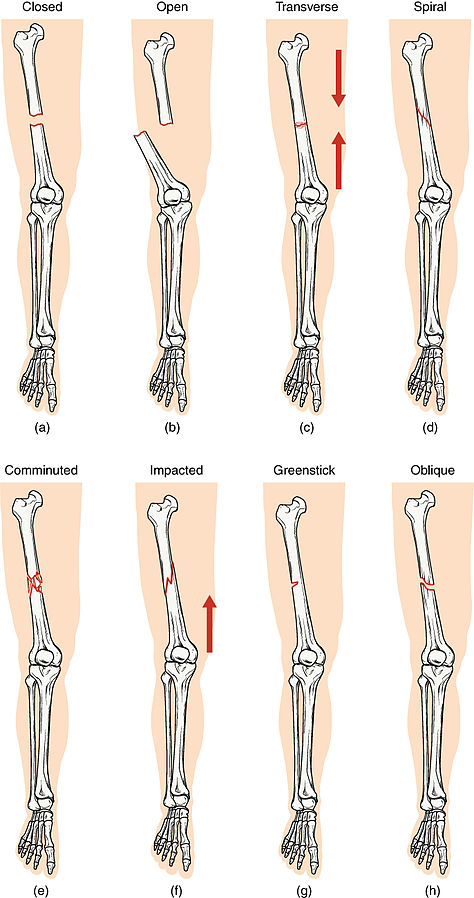 Illustration reference: OpenRN Health Alterations Ch.10.6.
Illustration reference: OpenRN Health Alterations Ch.10.6.
Risk Factors
- Advancing age and fall trauma.
- Fracture risk spans all age and sex groups, but older adults carry higher risk for major hip-fracture events.
- osteoporosis-bone-density-loss-and-fragility-fracture-risk, metastatic cancer, and endocrine disease burden (for example Cushing-related bone fragility).
- Long-term corticosteroid exposure.
- Low physical activity and reduced weight-bearing exercise.
- Poor nutrition and genetic susceptibility.
- Postmenopausal status with hormonally mediated bone-density decline.
Bone Healing Stages
- Hematoma formation (about 48-72 hours): Ruptured vessels form clot scaffold at fracture site.
- Hematoma to granulation tissue: Vascular and cellular infiltration clears damaged tissue.
- Callus formation: Collagen-cartilage soft callus stabilizes fracture ends.
- Osteoblastic proliferation: Woven bone progressively replaces soft callus.
- Bone remodeling: Woven bone matures into stronger lamellar structure.
- Healing completion: Often about 6 weeks, but can extend toward 6 months in higher-risk contexts.
Nursing Assessment
NCLEX Focus
Early priority is identifying unstable fracture patterns and protecting neurovascular function.
- Assess mechanism of injury and probable force pattern.
- Assess fracture type cues (open vs closed, displacement, fragmentation, partial vs complete).
- Assess pain, deformity, swelling, and movement limitation.
- Assess distal circulation, sensation, and movement for limb-threatening compromise.
- In suspected hip fracture, assess inability to bear weight, inability to lift/rotate limb, bruising/swelling, leg shortening, and external rotation.
- Assess multisystem findings:
- Musculoskeletal: localized tenderness, crepitus, deformity, limited ROM.
- Integumentary: bruising, bleeding/hematoma, wound or skin break, erythema/warmth.
- Nervous/cardiovascular: numbness, weakness, pallor, coolness, delayed capillary refill, decreased distal pulses.
- Respiratory/GI: rib-fracture-related shallow breathing and pain-related nausea/vomiting.
- Psychosocial: anxiety, distress, and ADL-function disruption.
Potential Complications
- Acute compartment syndrome (ACS): Pressure rise within muscle compartment causes ischemia-edema cycle and threatens irreversible muscle/nerve injury.
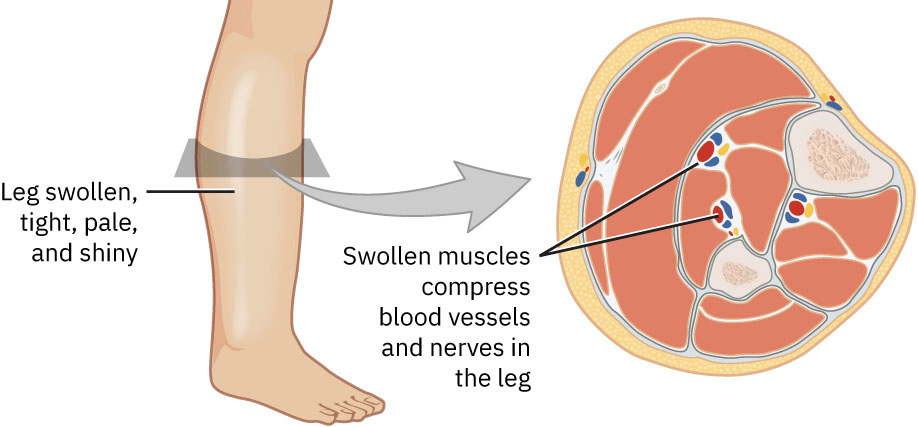 Illustration reference: OpenStax Medical-Surgical Nursing Ch.13.4.
Illustration reference: OpenStax Medical-Surgical Nursing Ch.13.4.
- Six P’s of ACS warning signs: Pain out of proportion, paresthesia, poikilothermia, pallor, pulselessness, and paralysis.
- ACS treatment context: Urgent cast release when tight casting is contributory and potential emergency fasciotomy for pressure decompression.
- Other major complications: Hypovolemic shock, fat embolism syndrome, DVT, infection, and delayed/nonunion-malunion healing.
- Fat embolism high-risk window: Most concerning about 24-72 hours after long-bone fracture (especially femur).
- Fat embolism cues: Respiratory distress, altered mental status, petechial rash, and fever; escalate emergently.
- DVT prevention context: Early mobilization, anticoagulants, and compression stockings when indicated.
Diagnostic Testing
- X-ray is the most common first-line test for fracture location and extent.
- CT helps define complex fractures and surrounding structural detail.
- MRI supports subtle fracture and soft-tissue/ligament-tendon evaluation.
- Ultrasound can improve growth-plate visualization in pediatric fracture contexts.
- Bone scan may be used when metastatic disease is suspected as fracture etiology.
Nursing Interventions
- Stabilize and protect the injured area while avoiding unnecessary movement.
- Escalate open-fracture findings and neurovascular deterioration urgently.
- Perform frequent distal neurovascular checks and trend the 5 P findings (pain, pulse, pallor, paresthesia, paralysis).
- Prepare for imaging, reduction, and immobilization workflow based on ordered plan.
- In hip fracture contexts, anticipate time-sensitive surgical planning (often within about 48 hours) with ORIF or arthroplasty pathways.
- Reinforce injury-protection and follow-up expectations.
- Monitor for ACS and immediately escalate six-P progression or worsening perfusion/sensation.
- For suspected fat embolism deterioration, notify the provider urgently, activate rapid-response workflow when indicated, and initiate oxygen support while preparing for higher-acuity airway support.
- Reinforce DVT prevention measures and monitor for unilateral swelling, warmth, redness, and pain.
- Reinforce prescribed mobility/ROM exercises that remain safe while cast or splint support is in place.
Fracture Reduction and Stabilization
- Closed reduction: Nonsurgical manual realignment followed by cast/splint/brace immobilization.
- Closed-reduction comfort support: Local anesthetic/sedative/analgesic combinations are commonly used because realignment can be very painful.
- ORIF (open reduction internal fixation): Surgical realignment with internal hardware (pins, plates, rods, screws); hardware is often left in place unless symptoms require removal.
- External fixation: Percutaneous pins/wires above and below fracture connected to an external frame; commonly used for open fractures, heavily contaminated wound contexts, and selected pelvic fractures, often as temporary stabilization.
- Arthroplasty in selected joint fractures: Severe fracture patterns involving major joints (for example shoulder, elbow, hip, or knee) may require joint-replacement surgery.
Immobilization and Traction
- Immobilization with cast, splint, or brace restricts movement to support bone alignment and healing.
- Cast/splint immobilization duration is often about 3-8 weeks, depending on fracture site and severity.
- Traction may be used to align fracture and reduce muscle spasm via controlled pull and countertraction.
- Traction force is applied slowly and steadily, commonly through rope-pulley-weight systems that maintain continuous alignment tension.
- Skin (Buck’s) traction: Weights and boot setup, often temporary until surgery or definitive reduction.
- Skeletal traction: Pins, wires, or screws are inserted in bone distal to the fracture and connected to traction weights for realignment.
- In polytrauma with multiple fractures, skeletal traction may be used before surgery to improve alignment while other injuries are stabilized.
- Traction-care priorities include continuously suspended freely hanging weights, intact rope/pulley system, alignment checks, skin protection, pin-site aseptic care, and frequent distal neurovascular reassessment.
- External-fixator pin-site care includes gentle daily cleansing and careful drying (avoid rubbing/friction) plus prompt reporting of redness, drainage, swelling, or worsening pain.
- Provide or position ordered trapeze support when available to aid safer independent repositioning without disrupting traction alignment.
Health Teaching
- Apply provider-ordered ice/cold packs for about 10-20 minutes at a time, commonly every 1-2 hours while awake during early swelling phases.
- Elevate injured extremity near heart level when appropriate to reduce swelling and discomfort.
- Reinforce safe use of assistive devices, casts, splints, and progressive ROM/ambulation plan.
- Cast teaching: keep cast dry, avoid inserting objects into cast, inspect edges/skin, and report numbness, tingling, color change, foul odor, drainage, worsening pain, or perfusion changes.
- For non-waterproof casts, cover the cast during showers to keep plaster material dry and preserve fit.
- For external-fixation care, teach daily pin/wound observation and prompt reporting of redness, warmth, swelling, drainage, or worsening pain suggestive of infection risk (including osteomyelitis).
- After cast/splint removal, expect reassessment for deformity, swelling, pain, distal movement, distal pulse/perfusion, and follow-up x-ray healing status.
- Reinforce a balanced diet with adequate protein intake to support tissue and bone healing.
Complication Escalation
Open fractures and worsening distal neurovascular findings require immediate escalation to prevent permanent harm.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| analgesics | Opioids, local anesthetic contexts | Use adequate pain control to support assessment and safe positioning. |
| nsaids | ibuprofen-class contexts | nsaids (NSAIDs) may be limited/avoided in selected fracture-healing plans because of malunion concern. |
| antibiotics | Open-fracture and postoperative contexts | Early infection-risk management is critical when skin integrity is disrupted. |
| anticoagulants | Post-fracture prophylaxis contexts | Support DVT prevention during reduced mobility phases after fracture/surgery. |
Clinical Judgment Application
Clinical Scenario
A patient presents after a fall with severe forearm pain, visible deformity, and an overlying skin wound with bone exposure.
- Recognize Cues: Open fracture with high contamination risk.
- Analyze Cues: Immediate priorities are infection prevention, stabilization, and neurovascular preservation.
- Prioritize Hypotheses: Limb viability and systemic infection prevention are urgent.
- Generate Solutions: Protect wound, initiate urgent escalation, and prepare for reduction/definitive care.
- Take Action: Perform focused distal checks, support ordered interventions, and document trend findings.
- Evaluate Outcomes: Neurovascular status remains stable and definitive fracture management proceeds safely.
Related Concepts
- musculoskeletal-physical-assessment-and-functional-mobility - Injury-focused assessment and neurovascular red-flag detection.
- immobilization-devices-and-restraint-safety - Cast, splint, traction, and distal-check safety framework.
- fall-prevention - Prevention context for fracture recurrence risk reduction.
- musculoskeletal-system - Structure-function baseline for fracture interpretation.
- osteomyelitis - Bone-infection complication risk in open-fracture and fixation contexts.
- deep-vein-thrombosis - Post-fracture immobility complication and prophylaxis context.
Self-Check
- Why does open versus closed fracture classification change urgency?
- Which fracture patterns most strongly suggest unstable injury burden?
- Which distal findings indicate emergent neurovascular compromise?