Musculoskeletal System
Key Points
- The musculoskeletal system enables movement, posture, organ protection, and mineral storage.
- Purposeful activity depends on coordinated skeletal, muscular, joint, and central-nervous-system signaling.
- Connective tissues (ligaments, tendons, cartilage) coordinate force transfer and joint stability.
- Activity, range-of-motion work, and nutrition support are central to preserving function and preventing decline.
Pathophysiology
The musculoskeletal system integrates bones, joints, muscles, and connective tissues to generate movement and maintain structural integrity. Skeletal muscle contracts and transfers force through tendons to bones, while ligaments and cartilage maintain alignment and reduce friction stress across joints. Cardiac, smooth, and skeletal muscle all share excitability, where membrane depolarization produces an action-potential signal. Skeletal muscle depends on nervous-system signaling for contraction, whereas cardiac and smooth muscle can also respond to autonomic, hormonal, and local stimuli.
The adult skeleton contains about 206 bones. In addition to support, movement, and organ protection, skeletal structures contribute to hematopoiesis and mineral/fat storage-homeostasis.
Tendons are dense collagenous continuations of muscle sheaths that anchor to bone coverings and transmit contractile force as levered movement. They also absorb part of impact load during high-force activity, but relatively low tendon perfusion contributes to slower healing after injury.
In biomechanical terms, bones act as levers and joints function as hinges/pivots that convert muscle force into movement. Musculoskeletal functional emphasis shifts across the lifespan as support, movement demand, and metabolic reserve needs change.
Joint motion capacity spans near-immobile (synarthrosis), limited-mobility (amphiarthrosis), and freely movable (diarthrosis) patterns. Most highly mobile joints are synovial joints, where synovial fluid and articular cartilage reduce friction during repeated motion.
Voluntary movement control depends on central processing (brain/spinal cord), peripheral nerve transmission, and somatic motor signaling to skeletal muscle. Spinal nerves distribute sensory input and motor commands throughout the body, and neuromuscular junctions translate motor-neuron signals into skeletal-muscle contraction.
Functional decline occurs with inactivity, aging, pain-avoidance behavior, and chronic inflammatory or degenerative disease. Reduced mobility accelerates weakness, stiffness, fall risk, and loss of independence in activities of daily living. Sustained faulty posture increases joint stress and can progressively worsen spinal alignment, neck-shoulder-back pain, flexibility, balance, and fall risk; over time it may also contribute to respiratory and digestive inefficiency.
Pediatric musculoskeletal patterns differ from adults in clinically important ways: children have more bones before fusion with growth, infant tone and coordination are less mature and require handling support, pediatric bones are more flexible (can sustain significant injury with limited visible fracture), and growth-plate injury can alter long-bone development.
Impaired musculoskeletal function often produces predictable multisystem effects: inflammatory-response signs (pain, heat, redness, swelling, loss of function), reduced dexterity/mobility, electrolyte disturbances (especially calcium/phosphorus context), altered marrow-related blood-cell production, fatigue, and ADL limitation. Psychological effects commonly include anxiety/depression, reduced social/work participation, and sleep disruption related to persistent pain or function loss.
Bone is metabolically active tissue. Osteoblasts form bone, osteoclasts resorb bone, and osteocytes maintain mature matrix. The ongoing remodeling balance supports skeletal strength and calcium homeostasis; imbalance contributes to osteopenia and osteoporosis-bone-density-loss-and-fragility-fracture-risk.
Skeletal development begins from embryonic fibrous and cartilaginous templates, with ossification starting early in gestation and continuing through young adulthood (commonly into the mid-20s). Normal lifelong bone health depends on balanced ossification and resorption.
Bone marrow supports hematopoiesis. Red marrow generates erythrocytes, leukocytes, and platelets, whereas yellow marrow is adipose-rich energy reserve tissue.
Bone matrix serves as a calcium/phosphorus reservoir that supports neuromuscular signaling and contraction physiology when circulating levels need buffering.
Muscles act in coordinated agonist-antagonist patterns: one group contracts while another relaxes to produce controlled motion. Core movement terms include flexion, extension, abduction, adduction, circumduction, rotation, pronation/supination, dorsiflexion/plantar flexion, inversion/eversion, and scapular or mandibular protraction/retraction/elevation/depression.
Purposeful movement is typically organized around a prime mover, aided by synergists and balanced by antagonists that preserve alignment and return joints toward neutral. With inactivity, skeletal muscle atrophy reduces both strength and movement tolerance. Postural reflexes are continuous involuntary adjustments integrating neuromuscular control with vestibular and visual input to maintain alignment and prevent falls during expected and unexpected movement demands.
Classification
- Skeletal framework: Bones and joints for support, protection, and leverage.
- Activity-alignment domain: Safe purposeful movement requires proper body positioning (alignment) before and during activity.
- Bone-shape functional types:
- Long bones: Provide leverage for movement (for example femur/humerus).
- Short bones: Improve stability with limited motion (for example carpals/tarsals).
- Flat bones: Protect organs and provide broad muscle-attachment surfaces.
- Sesamoid bones: Embedded in tendons to reduce stress and improve force mechanics.
- Irregular bones: Mixed-form support/protection structures (for example vertebrae).
- Regional functional specialization: Lower-limb structures prioritize weight-bearing stability and gait, while upper-limb structures prioritize mobility and object manipulation.
- Muscle components: Voluntary skeletal muscle and involuntary smooth/cardiac muscle roles.
- Neural-control layers: Central nervous system processing, peripheral nerve pathways, and somatic motor output for purposeful movement.
- Neuromuscular transmission unit: Sensory neurons, motor neurons, and neuromuscular-junction signaling that initiates or stops contraction.
- Connective-tissue roles: Ligament stability, tendon force transfer, and cartilage cushioning.
- Tendon-risk context: Traumatic load and selected medication exposures (for example fluoroquinolone-class antibiotics) can increase tendon injury or rupture risk.
- Ligament healing constraint: Ligaments have lower perfusion than bone, so ligament injuries often heal more slowly and require longer protection/rehabilitation timelines.
- Motor-function categories: Gross motor movement (trunk/legs) and fine motor movement (hands/wrists) for daily-function tasks.
- Common chronic condition context: Osteoarthritis-related pain and movement limitation.
- Skeletal divisions:
- Axial skeleton: Cranium/facial bones, hyoid, vertebral column, and thoracic cage that protect brain, spinal cord, heart, and lungs.
- Appendicular skeleton: Upper and lower limbs with shoulder and pelvic girdle attachments.
- Vertebral organization: Cervical (C1-C7), thoracic (T1-T12), lumbar (L1-L5), sacrum, and coccyx with intervertebral discs for shock absorption and flexibility.
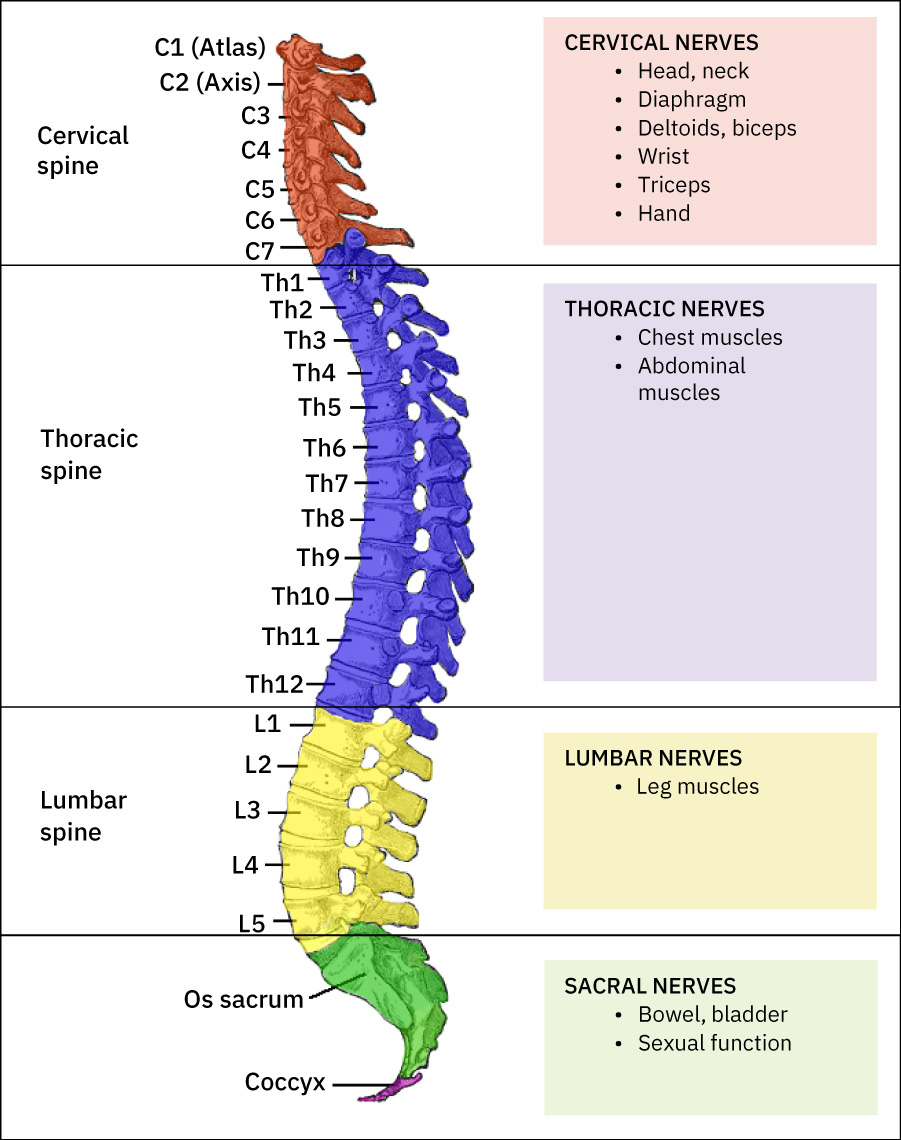 Illustration reference: OpenStax Clinical Nursing Skills Ch.26.1.
Illustration reference: OpenStax Clinical Nursing Skills Ch.26.1.
- Thoracic cage structure: Sternum with true ribs (1-7), false ribs (8-10), and floating ribs (11-12).
- Upper-limb structure: Humerus, radius, ulna, carpals, metacarpals, and phalanges with clavicle/scapula/acromion shoulder support.
- Lower-limb structure: Femur, patella, tibia, fibula, tarsals, metatarsals, phalanges, and calcaneus with pelvic acetabular articulation.
- Joint-structure categories:
- Fibrous joints: Minimal/no movement (for example skull sutures).
- Cartilaginous joints: Slight movement (for example pubic symphysis, intervertebral discs).
- Joint-mobility classes:
- Synarthrosis: Unmovable or nearly unmovable joints.
- Amphiarthrosis: Limited-motion joints.
- Diarthrosis: Freely movable joints (most are synovial).
- Synovial joints: Freely movable joints with joint cavity, synovial membrane, and synovial fluid.
- Synovial-joint types: Pivot, hinge, condyloid, saddle, plane, and ball-and-socket.
- Synovial friction-control components: Articular cartilage plus synovial fluid for low-friction movement.
- Intra-articular support structures: Menisci/articular discs, ligaments, tendons, and additional cartilage that stabilize and distribute load.
- Joint tradeoff principle: Greater mobility often means lower inherent stability and higher injury susceptibility.
- Muscle-tissue types:
- Smooth muscle: Involuntary contraction in organ walls.
- Cardiac muscle: Involuntary striated contractile tissue of the heart.
- Skeletal muscle: Voluntary striated muscle that drives posture and movement.
- Muscle-atrophy patterns:
- Physiologic atrophy: Disuse-related loss that may improve with activity and nutrition support.
- Pathologic atrophy: Disease/aging/starvation or long-term corticosteroid-associated loss.
- Neurogenic atrophy: Nerve-injury-related severe loss requiring prompt neurologic evaluation and rehabilitation planning.
- Cardiac-muscle control: Specialized pacemaker cells set rhythm and respond to ANS/hormonal modulation.
- Smooth-muscle distribution: Found in hollow organs and vessel/airway walls, with additional iris/lens and piloerector control roles.
- Skeletal-muscle physiology: Striated fibers contain sarcomeres built from actin and myosin, enabling contraction, heat generation, and movement support.
- Functional extras of skeletal muscle: Supports swallowing/elimination control at selected tract openings, protects internal organs, and helps venous return during ambulation.
- Functional movement-role categories:
- Prime mover (agonist): Main muscle generating a movement.
- Synergist: Muscle assisting or stabilizing the prime mover.
- Antagonist: Muscle producing the opposite action to control alignment and return.
Articular cartilage and synovial lubrication minimize friction during movement, but degeneration or trauma can damage these low-friction surfaces and reduce function. In clinical care, knee, hip, and shoulder joints are frequent injury/problem sites because they combine high load or high range-of-motion demand.
Nursing Assessment
NCLEX Focus
Priority questions emphasize identifying mobility decline early and selecting interventions that preserve independence safely.
- Assess gait stability, transfer ability, endurance, and pain-limited movement.
- Observe joint stiffness, swelling, and reduced range of motion affecting ADLs.
- Interpret joint sounds in context: activity-related painless crepitus is often benign, but crepitus with pain, swelling, or recent injury requires escalation.
- Identify fall-risk cues linked to weakness, balance deficits, or delayed reaction time.
- Assess for classic inflammation pattern changes (pain, heat, redness, swelling, loss of function) in injured or painful areas.
- Assess psychosocial impact of function loss, including reduced participation, mood symptoms, and insomnia.
- Report new pain patterns, acute function decline, or inability to perform baseline tasks.
Nursing Interventions
- Encourage ambulation and weight-bearing activity as tolerated to preserve bone/muscle health.
- Support scheduled range-of-motion activities and safe positioning routines.
- Apply comfort measures for chronic joint pain (heat/ice, massage, repositioning per plan).
- Individualize osteoarthritis comfort measures because response to ice/heat/topicals/repositioning varies by resident preference and tolerance.
- Reinforce nutrition patterns supporting tissue repair and bone health (protein and calcium intake).
Deconditioning Spiral
Avoidable inactivity rapidly worsens weakness and fall risk; early mobility support is a high-value safety intervention.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| nsaids | Osteoarthritis symptom-control context | Monitor comfort response and report persistent functional pain limits. |
| nsaids (topical-analgesics) | Local pain-relief context | Useful adjuncts to improve participation in mobility activities. |
Clinical Judgment Application
Clinical Scenario
A resident with osteoarthritis reports worsening knee pain and begins refusing ambulation over several days.
- Recognize Cues: Increasing pain, reduced activity, and early functional withdrawal.
- Analyze Cues: Reduced mobility is likely to accelerate weakness and dependence.
- Prioritize Hypotheses: Immediate priority is preserving safe movement while controlling discomfort.
- Generate Solutions: Use comfort measures, paced ambulation, and assisted ROM schedule.
- Take Action: Implement support plan and communicate trend changes to nurse.
- Evaluate Outcomes: Mobility participation improves and fall-risk behaviors decrease.
Related Concepts
- immobility-complications - Inactivity drives multisystem decline and functional loss.
- fall-prevention - Mobility deficits and pain increase transfer/ambulation injury risk.
- osteoarthritis-degenerative-joint-disease - Degenerative joint-disease context for chronic pain, stiffness, and function decline.
- osteomyelitis - Bone-infection pattern with prolonged antibiotic and possible surgical source-control needs.
- osteoporosis-bone-density-loss-and-fragility-fracture-risk - Progressive bone-density loss and fragility-fracture context.
- range-of-motion-exercises-for-the-shoulder - Core intervention for maintaining flexibility and joint function.
- safe-patient-transfer - Proper mechanics protect both client and caregiver.
- enteral-nutrition-support - Protein and micronutrient intake support tissue repair and strength.
Self-Check
- Which findings suggest musculoskeletal decline is becoming a fall-risk emergency?
- How does joint pain contribute to the deconditioning cycle?
- Which daily interventions best preserve mobility and ADL independence?