Common Musculoskeletal Disorders Recognition and Care Priorities
Key Points
- Common disorders include spinal alignment abnormalities, inflammatory/degenerative joint disease, tendon disorders, and foot deformities.
- Early pattern recognition supports functional preservation and prevention of avoidable disability.
- Severe neurologic deficits, acute ischemic signs, or rapid functional decline require urgent escalation.
Pathophysiology
Musculoskeletal disorders arise from congenital variation, repetitive mechanical stress, inflammatory or autoimmune processes, trauma, metabolic imbalance, and aging-related degeneration. These mechanisms alter alignment, load transfer, and joint function.
Persistent inflammation and structural breakdown can progress from pain and stiffness to deformity, mobility loss, and decreased ADL independence.
Spinal disorders can alter normal curve mechanics that support upright posture and shock dissipation. As alignment worsens, compensatory muscle/posture patterns may increase fatigue, pain, neurologic symptoms (for example paresthesia/weakness), and dependency in daily activities.
Classification
- Spinal disorders: Flatback syndrome, hyperlordosis, kyphosis, scoliosis, and ankylosing spondylitis patterns.
- Flatback pattern context: Loss of normal lumbar lordosis can drive compensatory hip/cervical extension and knee flexion with progressive end-of-day fatigue and pain; etiologies include prior spinal surgery, congenital variation, degeneration, trauma, osteoporosis, and compression-fracture history.
- Bone-alignment disorders: Fracture/dislocation malalignment, intoeing, selected growth-plate disorders (for example Blount disease), and accessory-bone variants that may alter gait/load distribution.
- Joint and bone disorders: osteoarthritis-degenerative-joint-disease, rheumatoid-arthritis-autoimmune-joint-disease, and osteoporosis-bone-density-loss-and-fragility-fracture-risk.
- Traumatic bone disorders: Fracture patterns requiring reduction, immobilization, and neurovascular surveillance.
- Bone-shape/structure disorders: Degenerative spurring, cystic change, post-surgical structural variation, and neoplastic/metastatic reshaping.
- Bone-length discrepancy disorders: Congenital, infectious, traumatic, or neoplastic growth effects causing clinically meaningful limb-length difference.
- Neoplastic bone disorders: Primary bone malignancies (osteosarcoma, Ewing sarcoma, chondrosarcoma) and metastatic bone involvement.
- Neurodevelopmental movement disorders: Cerebral palsy patterns with spasticity, dyskinesia, or ataxia that alter long-term mobility needs.
- Wrist-hand disorders: Ganglion cyst, tenosynovitis, and carpal tunnel syndrome.
- Foot-toe disorders: gout, pes planus, hallux valgus, and hammertoe.
Additional Disorder Snapshots
- Ankylosing spondylitis: Inflammatory axial-spine disease often presenting with chronic, gradual-onset back pain before age 40 that improves with activity and may worsen at night; monitor urgently for spinal-cord compression or cauda-equina pattern (new extremity numbness/weakness, coordination loss, foot drop, or new bowel/bladder dysfunction).
- Bone cancer: Suspect with persistent bone pain/swelling, pathologic-fracture tendency, fatigue, and unintended weight loss; workup may include X-ray, CT/MRI, PET, bone scan, and biopsy with treatment based on stage/type.
- Cerebral palsy: Nonprogressive brain injury/development disorder causing persistent movement/posture impairment (spasticity, dyskinesia, or ataxia) and requiring individualized long-term multidisciplinary support.
- Clubfoot (congenital talipes): Congenital inward/downward foot-position deformity treated early with serial casting; severe cases may require surgery followed by prolonged brace support.
- Dislocation/subluxation: Complete or partial joint displacement presents with severe pain, swelling, deformity, and movement loss; requires prompt reduction and post-reduction stabilization/rehabilitation, with elevated recurrence risk.
- Fibromyalgia: Central pain-processing sensitivity disorder with widespread pain, fatigue, sleep/cognitive symptoms, and mood comorbidity; management is multimodal (exercise, education, stress/sleep optimization, and selected medications/CBT).
- Foot drop: Inability to dorsiflex the foot from neuromuscular weakness/paralysis; gait compensation is common, and treatment often uses AFO-style bracing plus gait-strengthening therapy.
- Ganglion cyst: Fluid-filled cyst most often on the dorsal wrist over tendon sheath or joint; common in women, people roughly 15-40 years old, and repetitive wrist-load groups (for example gymnastic activity). Some resolve with rest/splinting; aspiration may relieve pain but recurrence is common, and persistent symptomatic cases may need surgical excision.
- gout: Inflammatory crystal arthropathy from hyperuricemia (urate crystal deposition), commonly with recurrent flares in the great toe/lower limb; treatment commonly includes NSAIDs/colchicine for flares and allopurinol for recurrent hyperuricemia control.
- osteomyelitis: Bone infection from hematogenous spread, contiguous tissue spread, or direct inoculation; diabetes/foot-ulcer and smoking comorbidity increase risk, and treatment often requires prolonged IV antibiotics with possible surgery.
- Osteoarthritis (DJD): Age-related degenerative joint disease from repetitive inflammation-cartilage loss cycles, most often affecting weight-bearing joints (spine/hips/knees) and also fingers; risk increases with obesity, family history, and prior overuse/injury, with higher prevalence in women after about age 50.
- Osteoporosis: Progressive bone-density loss causing fragility-fracture risk (especially hip, spine, and wrist); prevention and care emphasize calcium/vitamin D intake, weight-bearing activity, smoking avoidance, and medication therapy (for example bisphosphonate/calcitonin contexts) when fracture risk is high.
- Muscular dystrophy (including DMD): Rare inherited progressive muscle disorders with more than 30 subtypes and wide variation in onset/severity; mobility loss, contracture risk, scoliosis-related pulmonary decline, and eventual dependence in walking/ADLs are common long-term trajectories requiring multidisciplinary care.
- Paralysis syndromes: Pattern-based distribution includes hemiplegia, paraplegia, and tetraplegia, with flaccid versus spastic muscle effects; long-term care emphasizes rehabilitation services and adaptive/assistive technology for independence.
- Pes planus (flat feet): Loss of the medial longitudinal foot arch; common in early childhood before arch development and associated in later life with obesity, posterior tibial tendon dysfunction, or tight Achilles/calf structures. Findings include weight-bearing arch collapse, altered gait, and back/leg/ankle/foot pain. Management may include NSAIDs, orthotics, motion-control footwear, weight reduction support, and surgery for refractory severe deformity.
- Hallux valgus (bunion): Medial bony protrusion at the first metatarsophalangeal joint with progressive inward deviation of the great toe toward adjacent toes; associated with hereditary patterns, autoimmune/inflammatory joint disease contexts (for example RA), and chronic tight-restrictive footwear. Common findings include deformity with erythema/edema, callus burden, pain or numbness, and walking difficulty; management includes NSAIDs, ice, orthotics, footwear adjustment, PT, selected steroid injection, and bunionectomy in severe cases.
- Hammertoe: Flexion deformity at the proximal interphalangeal region (often second toe) with hammer-like contour; associated with trauma, hallux valgus, arthritis, congenital variants, and poor shoe fit, with higher prevalence in women. Corn/callus formation and painful gait are common clinical cues. Early PT-guided exercises with taping/splinting can reduce progression to fixed deformity; symptom relief may include intermittent ice, NSAIDs, or selected corticosteroid injection, with surgery for refractory deformity.
- rhabdomyolysis-muscle-breakdown-and-acute-kidney-injury-risk: Acute muscle-breakdown syndrome with myoglobin-mediated renal injury risk, requiring rapid fluid-resuscitation and renal monitoring.
- soft-tissue-injuries: Sprain/strain/contusion/tendinitis/bursitis patterns are commonly managed with early RICE, activity modification, and follow-up when recovery is delayed.
- Tenosynovitis (including De Quervain and trigger finger): Tendon-sheath inflammation can follow overuse, autoimmune disease (for example RA), or infection (including skin-flora pathogens such as S. aureus and MRSA). De Quervain pattern causes thumb-side wrist pain with grip/fist/turning motions and is often treated with splinting, NSAIDs, activity modification, steroid injection, or sheath-release surgery. Stenosing tenosynovitis (trigger finger) causes locking/clicking of a flexed digit and is more common with diabetes and older age.
- Vertebral-curvature disorders: Kyphosis, lordosis, and scoliosis alter spinal alignment and pain/function risk; management ranges from monitoring to bracing or surgery based on severity, progression risk, and neurologic impact.
- Scoliosis in school-age/adolescence: Lateral spinal curvature may present with asymmetric shoulder/hip height, scapular prominence, and rib-height asymmetry on forward bend; evaluation includes spinal imaging, and management ranges from observation to bracing, PT, or surgery based on growth status and curve severity.
- Hyperlordosis (swayback) pattern: Exaggerated lumbar curve with anterior abdominal and posterior pelvic prominence can cause neck/low-back pain; causes include obesity, pregnancy, prolonged posture strain, high-heel use, core weakness, and selected neuromuscular or structural disorders.
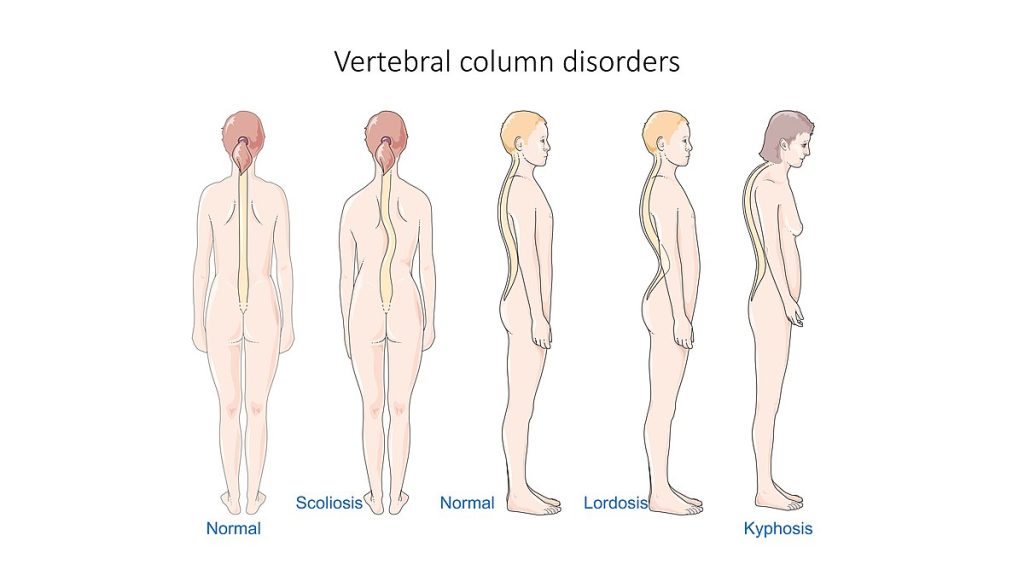 Illustration reference: OpenRN Health Alterations Ch.10.10.
Illustration reference: OpenRN Health Alterations Ch.10.10.
Nursing Assessment
NCLEX Focus
Prioritize symptoms that indicate threatened neurologic function, severe inflammation, or rapid mobility decline.
- Assess pain pattern, stiffness, swelling, deformity progression, and activity-related limitations.
- In chronic back-pain patterns, assess for inflammatory features (younger onset, gradual chronicity, night worsening, and improvement with movement rather than rest).
- Assess spinal posture and alignment changes with gait and balance impact.
- Assess hand/wrist sensory deficits, weakness, and repetitive-use associations.
- Assess foot pain, joint erythema/heat, shoe-pressure effects, and weight-bearing tolerance.
- Escalate immediately for new spinal-cord or cauda-equina cues (progressive extremity numbness/weakness, foot drop, coordination loss, or bowel/bladder dysfunction).
Nursing Interventions
- Escalate new neurologic deficits, bowel/bladder changes, severe inflammatory flare signs, or abrupt function loss.
- Reinforce condition-specific self-management (activity modification, footwear support, and medication adherence).
- Reinforce DJD and osteoporosis self-management: low-impact activity, weight optimization, fall prevention, and adherence to bone/joint medication plans.
- Coordinate physical therapy, assistive-device planning, and follow-up for progressive disorders.
Irreversible Function-Loss Risk
Delayed response to neurologic compromise, severe inflammation, or progressive deformity can cause permanent functional impairment.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| nsaids | Ibuprofen, naproxen contexts | Commonly used for inflammatory pain; monitor response and adverse effects. |
| disease-modifying-antirheumatic-drugs | Methotrexate-class contexts | Used in rheumatoid arthritis pathways; monitor for toxicity and infection risk. |
Clinical Judgment Application
Clinical Scenario
A patient with chronic back stiffness develops new leg numbness and worsening gait instability.
- Recognize Cues: Progressive neurologic deficits with functional deterioration.
- Analyze Cues: Pattern may indicate significant spinal involvement requiring urgent workup.
- Prioritize Hypotheses: Preventing neurologic injury and preserving mobility are immediate priorities.
- Generate Solutions: Initiate urgent escalation and safety-focused mobility support.
- Take Action: Document objective deficits and activate appropriate referral pathway.
- Evaluate Outcomes: Early intervention limits progression and supports recovery planning.
Related Concepts
- musculoskeletal-system - Structural and functional baseline for disorder interpretation.
- osteomyelitis - Bone infection recognition, diagnostics, and prolonged-treatment priorities.
- osteoarthritis-degenerative-joint-disease - Degenerative joint disease progression, diagnostics, and treatment pathways.
- musculoskeletal-physical-assessment-and-functional-mobility - Assessment sequence and red-flag detection.
- fracture - Type-based fracture recognition, complications, and treatment pathway.
- osteoporosis-bone-density-loss-and-fragility-fracture-risk - Bone-density loss pattern and fragility-fracture prevention priorities.
- soft-tissue-injuries - Sprain/strain/contusion/tendinitis/bursitis assessment and RICE-centered care.
- carpal-tunnel-syndrome - Median-nerve compression pattern within wrist-hand disorders.
- promoting-joint-mobility-and-activity - Function-preserving activity strategies.
- immobility-complications - Disability progression risk when movement declines.
Self-Check
- Which musculoskeletal findings should be escalated as urgent neurologic risk?
- How do degenerative and autoimmune joint disorders differ in progression patterns?
- Why is early functional-support planning essential across common musculoskeletal disorders?