Osteoporosis Bone Density Loss and Fragility Fracture Risk
Key Points
- Osteopenia is reduced bone mass and can progress to osteoporosis.
- Osteoporosis reflects bone-density loss and structural deterioration that increase fragility fracture risk.
- Sarcopenia and bone loss can progress together as osteosarcopenia, compounding fall and fracture risk.
- Imbalance between bone resorption and bone formation drives progressive skeletal weakness.
- Hip, spine, and wrist fractures are common high-impact outcomes.
- U.S. burden remains high, with tens of millions affected by osteoporosis or osteopenia.
- Lifespan calcium and vitamin D adequacy is foundational: maternal intake supports fetal bone growth, and youth intake supports bone accrual through young adulthood.
Pathophysiology
Osteoporosis Bone Density Loss And Fragility Fracture Risk develops when bone resorption persistently exceeds bone formation. The resulting reduction in bone mineral density and microstructural strength increases fragility and lowers trauma threshold for fracture.
The condition is often progressive and may remain clinically silent until fracture occurs. Bone fragility most commonly presents in the hip, spine, and wrist.
Classification
- Osteopenia: Reduced bone mass with elevated future osteoporosis risk.
- Osteoporosis: More advanced structural bone compromise with marked fragility-fracture risk.
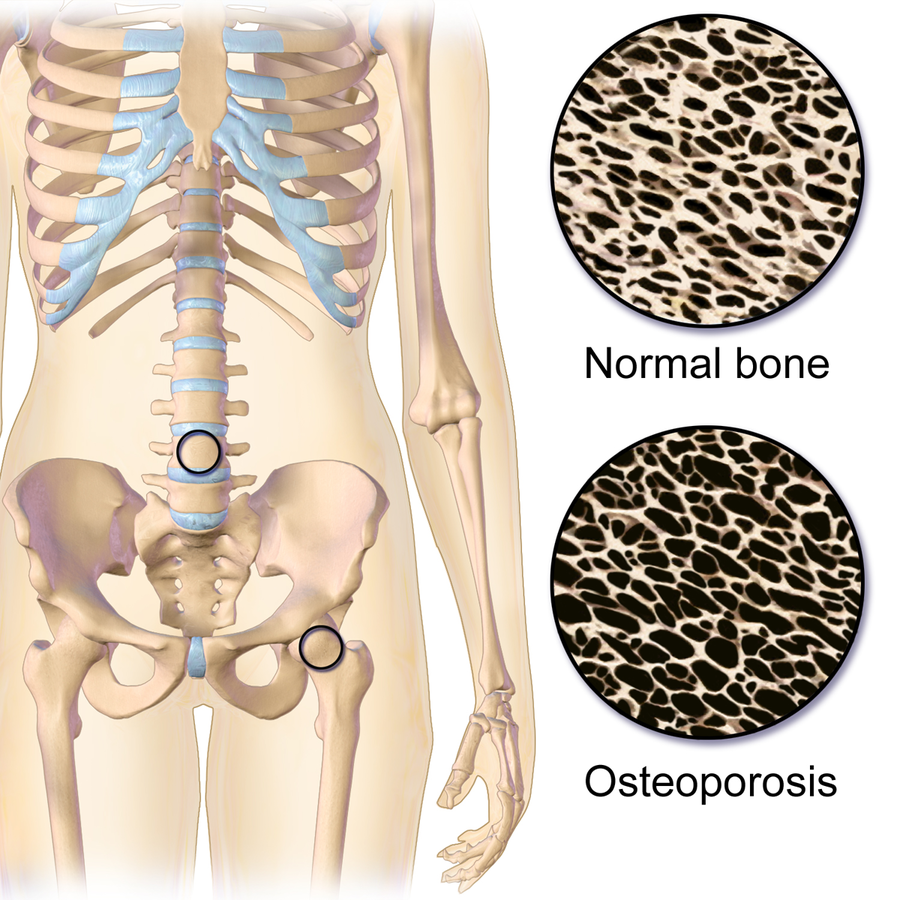 Illustration reference: OpenRN Health Alterations Ch.10.8.
Illustration reference: OpenRN Health Alterations Ch.10.8.
Risk Factors
- Advancing age.
- Female sex and postmenopausal hormone change.
- Genetic predisposition.
- Slender, thin-boned body frame and higher-risk ancestry patterns (for example Caucasian and Asian populations).
- Low body mass index and poor protein-calcium-vitamin-D intake patterns.
- Inadequate calcium and vitamin D intake.
- Comorbid disease burden (for example cancer, HIV, and anorexia nervosa pathways) that accelerates bone loss.
- Chronic corticosteroid exposure.
- Long-term use of selected medications including proton pump inhibitors and antiepileptic drugs.
- Selected inflammatory disorders such as rheumatoid arthritis.
- Smoking and excessive alcohol use.
- Low physical-activity and weight-bearing exercise patterns.
- Hormonal depletion states including low estrogen (for example menopause or excess exercise) and low testosterone in men.
- Midlife-to-older transition burden: osteoporosis prevalence is markedly higher in females over 50 (about 18.8%) than males over 50 (about 4.2%) in U.S. surveillance.
- Population burden context: about 54 million Americans live with osteoporosis and about 34 million with osteopenia.
Nursing Assessment
NCLEX Focus
Osteoporosis may remain asymptomatic until fracture; prioritize risk-pattern recognition and early fracture-prevention planning.
- Assess fracture history and low-trauma fracture patterns.
- Assess modifiable risk factors (nutrition deficits, smoking/alcohol, activity level).
- Assess medication and comorbidity contributors (for example chronic proton pump inhibitor therapy, rheumatoid arthritis, and endocrine hormone depletion states).
- Assess functional impact of fracture-related pain and mobility decline.
- Assess for reduced height, kyphosis, vertebral-compression signs, and hip/wrist fragility-fracture history.
- Assess for respiratory compromise when spinal deformity reduces chest expansion/lung capacity.
- Obtain baseline height and trend serial measurements over time to detect progressive vertebral-compression change.
Diagnostic Testing
- DEXA scan is the primary diagnostic test for bone density and fracture-risk stratification.
- Screening context: individuals assigned female at birth age
>=65should receive DXA screening; earlier testing is considered when risk burden is elevated. - T-score interpretation:
-1 to -2.5: osteopenia range.< -2.5: osteoporosis diagnostic range.
- QUS (quantitative ultrasound) at peripheral sites can support fracture-risk estimation.
- FRAX tool estimates 10-year hip-fracture and major-fracture probability to guide prevention intensity; common inputs include age, sex, height, weight, family history, and alcohol exposure.
- In later-stage osteoporosis, serial plain x-rays can help monitor disease progression.
- Lab values are not diagnostic for osteoporosis itself, but vitamin D, calcium, albumin, and phosphate are commonly trended to rule out alternate contributors.
Common Nursing Diagnoses
- Risk for injury.
- Impaired nutrition: less than body requirements.
Nursing Interventions
- Promote patient independence while assisting with ADLs as needed.
- Reinforce fracture-prevention and fall-risk reduction behaviors.
- Support nutrition and activity plans that protect bone health.
- Coordinate follow-up for bone-density evaluation and long-term risk management.
- In postmenopausal counseling contexts, reinforce daily intake targets of about
800 IUvitamin D and1,200 mgcalcium (combined diet plus supplements) when aligned with the prescribed plan. - For many adults, reinforce age-banded vitamin D targets (about
600 IU/daythrough age 70 and about800 IU/dayafter age 70) and calcium targets (often about1,200 mg/dayafter age 50) per the individualized plan. - Teach supplement safety: excessive calcium or vitamin D intake can increase risk of hypercalcemia, nephrolithiasis, and kidney injury, so clients should avoid unsupervised high-dose stacking from multiple fortified products and supplements.
- Include lifespan counseling when relevant: adequate maternal calcium/vitamin D in pregnancy and continued calcium/vitamin D support through childhood/adolescence to optimize peak bone mass.
- Provide health teaching on calcium/vitamin D food sources (for example dairy, leafy greens, fortified foods) and adherence to supplementation plans.
- Refer to a dietitian when calcium/vitamin-D intake gaps or nutrition barriers persist.
- Reinforce weight-bearing and resistance-exercise options aligned with client ability and preferences; consider PT referral for balance and exercise tailoring.
- Reinforce progressive weekly activity targets; combined aerobic, muscle-strengthening, and bone-loading activity totaling about 90 minutes per week can support bone-health outcomes in higher-risk adults.
- Clarify that weight-bearing activity (for example walking) is prioritized for bone-strength support, while non-weight-bearing exercise alone is usually insufficient for bone-loading goals.
- Teach safe sunlight strategies to support vitamin-D synthesis when appropriate (brief exposure with skin-protection precautions).
- Promote routine bone-density screening, especially in higher-risk groups such as postmenopausal women.
- Teach home fall-hazard reduction (for example rug removal, improved lighting, handrails) and safe assistive-device use.
Medical Management
- Pharmacotherapy is used to slow bone loss, support bone formation, and reduce fracture burden.
- Ensure vitamin-D insufficiency is corrected before or during bisphosphonate initiation when required by the treatment plan.
- Lifestyle treatment includes weight-bearing exercise, resistance training, calcium/vitamin D intake optimization, smoking cessation, and alcohol-risk reduction.
- Surgical options may be required for osteoporotic fractures (for example vertebroplasty for selected vertebral fracture stabilization).
Outcome Indicators
- Demonstrates improved understanding of diagnosis and treatment on pre/post education checks.
- Reports improved back-pain intensity on validated pain-scale reassessment.
- Remains free of new fragility fractures on interval follow-up.
- Verbalizes preferred calcium-rich food sources.
- Verbalizes concrete home modifications that reduce fall risk.
- Demonstrates adherence to bone-health and fracture-prevention plan.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| bisphosphonates | alendronate, risedronate, ibandronate | First-line antiresorptive context; monitor adherence and fracture-risk trend. |
| denosumab | denosumab injection (twice-yearly schedule context) | Supports antiresorptive pathway; monitor administration timing and adverse effects. |
| hormonal-therapy (selective-estrogen-receptor-modulators) | raloxifene | Postmenopausal bone-density support context; evaluate thrombosis-risk profile, smoking status, and prior DVT/PE history before use. |
| parathyroid hormone analogs | teriparatide, abaloparatide | Anabolic pathway to stimulate bone formation in selected high-risk clients. |
| calcitonin | calcitonin-class therapy | May support antiresorptive pain/bone-density goals in selected plans. |
| calcium and vitamin-D supplementation | oral supplementation contexts | Reinforces dietary deficits and improves mineralization support. |
Related Concepts
- musculoskeletal-system - Bone remodeling physiology context.
- musculoskeletal-physical-assessment-and-functional-mobility - Risk-focused assessment and mobility surveillance.
- fracture - Fragility-fracture outcomes and acute-care pathways.
- fall-prevention - Primary strategy to reduce osteoporotic injury burden.
Evaluation
- Reassess whether expected outcomes are met, partially met, or unmet in the planned timeframe.
- Revise care plan when education, nutrition, activity, or safety goals are not achieved.
- Repeat evaluation after interventions, new diagnostic/lab updates, and interprofessional plan changes.