Choking Maneuver and Airway Clearance
Key Points
- If the person can cough forcefully, encourage continued coughing while monitoring closely.
- If the person cannot cough, speak, or breathe, begin immediate airway-clearance intervention.
- Continue thrusts until object expulsion or unresponsiveness, then transition to CPR protocol.
Equipment
- No device required for immediate thrust technique
- Emergency call/alert access
- CPR support resources per facility protocol
Procedure Steps
- Recognize airway obstruction signs and immediately notify nurse or activate emergency response according to setting.
- If no nurse is available, direct another responder to call 911 while airway-clearance care continues.
- If the person is forcefully coughing, coach continued coughing and monitor deterioration.
- If the person cannot cough, speak, or breathe, state intent to assist and position behind the person.
- For standing adult, place one leg between victim’s legs for balance and reach around abdomen.
- For a child, move down to the child’s level and keep your head to one side during thrusts.
- Locate navel and place thumb side of fist above navel; grasp fist with other hand.
- Deliver quick inward-and-upward abdominal thrusts.
- For pregnant individuals, those you cannot get your arms around, or when abdominal thrusts are ineffective, deliver chest thrusts from behind while avoiding rib compression.
- If person is in wheelchair and cannot stand, lean forward safely and perform thrusts from behind.
- Continue thrusts until object is expelled or person becomes unresponsive.
- If unresponsive, notify nurse immediately; if no nurse is available, call 911 and initiate standard CPR sequence per training and policy.
- After relief of choking, seek medical evaluation and report event details to nurse.
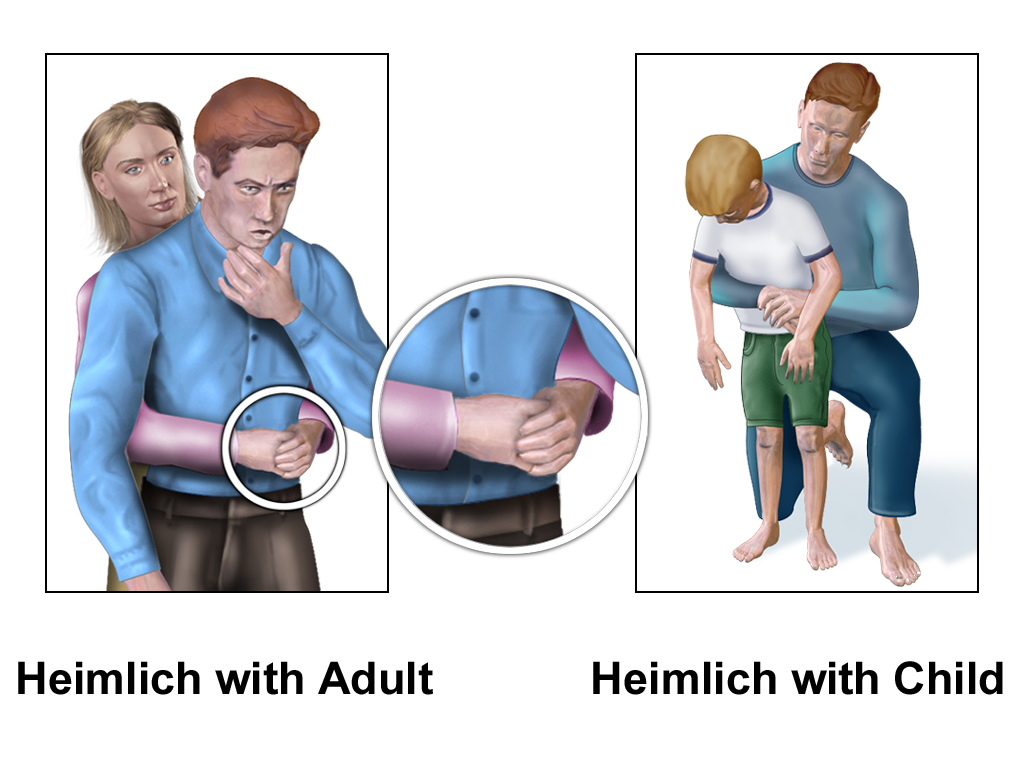 Illustration reference: OpenRN Nursing Assistant Ch.3.2.
Illustration reference: OpenRN Nursing Assistant Ch.3.2.
Common Errors
- Delaying intervention when speech and breathing are absent → increases hypoxia and arrest risk.
- Placing objects in mouth during distress → worsens obstruction and aspiration risk.
- Incorrect thrust location (too high/too low) → reduces effectiveness and can cause injury.
- Ending care without post-event medical evaluation → may miss residual airway injury or aspiration.
Related
- emergency-situations-and-rapid-response - Choking management is a core rapid-response scenario.
- communication-within-the-health-care-team - Immediate escalation and concise reporting improve outcomes.