Violence and Safety
Key Points
- Safety of clients and staff is a core psychiatric nursing priority.
- Most people with mental illness are not violent; risk is context-dependent and dynamic.
- Early cue recognition and therapeutic intervention reduce escalation and restrictive intervention use.
- Seclusion and restraint are legal-ethical last resorts with strict monitoring/documentation requirements.
- Workplace violence in health care can originate from patients, families/visitors, coworkers, or other personnel and requires organization-level prevention planning.
- Health care workers face substantial career-long violence exposure, so early agitation-cue recognition and team-based escalation pathways are critical.
Pathophysiology
Violence risk in psychiatric settings emerges from interacting factors including acute anxiety, fear, agitation, substance effects, environmental overstimulation, and unmet needs. Escalation often follows recognizable behavioral and physiologic cue patterns.
Proactive regulation support and person-centered approaches can interrupt escalation before harm occurs.
Classification
- Cue levels: Early anxiety/agitation, mid-level verbal aggression, and late-stage imminent violence.
- Intervention ladder: Verbal/relational interventions, PRN medication support, then restrictive emergency measures only if necessary.
- Time-out versus seclusion domain: Time-out is voluntary and the client can leave, while seclusion is staff-imposed protective confinement for emergency safety.
- Safety domains: Client safety, staff safety, environmental safety, and post-incident recovery/debriefing.
- Child maltreatment domains: Neglect, physical abuse, sexual abuse/exploitation, and emotional abuse.
- Abuse-form domain: Physical, psychological/emotional, sexual, and financial abuse can create overlapping immediate and long-term harm.
- Adolescent relationship-violence domain: Teen dating abuse patterns including coercion, assault, and stalking behaviors.
- Elder abuse/neglect domain: Harm by a trusted caregiver and failure to meet basic needs (food, water, shelter, hygiene, medical/dental care).
- Vulnerable-adult domain: Adults with physical or mental conditions that impair independent self-care have elevated abuse and exploitation risk.
- Community-violence domain: School bullying/cyberbullying and workplace violence (threats, intimidation, harassment, physical assault).
- Workplace violence sources: Patients, visitors/family members, coworkers, and other health system personnel.
- Workplace-pattern domain: Horizontal/lateral violence, client-on-worker violence, and incivility escalation patterns.
- Bias-targeted violence domain: Hate-crime risk affecting marginalized populations.
- At-risk population domain: Very young/older adults, disability or communication barriers, veterans, LGBTQIA+ groups, trafficking survivors, and socially marginalized groups.
- High-risk workflow periods: Mealtimes, shift changes, and transport transitions can increase disruptive behavior and escalation risk.
- Escalation-sequence domain: Some events follow anger to authority-resistance to confrontation progression, but medical/syndromic agitation can also become violent without warning.
Nursing Assessment
NCLEX Focus
Prioritize early recognition of agitation cues and immediate least-restrictive action planning.
-
Assess observable escalation cues (voice, posture, pacing, clenched hands, threat language).
-
Assess CDC-linked violence cues such as cursing or menacing tone, staring, panting, crossed arms, uncared-for appearance, intoxication signs, and throwing objects.
-
Assess anxiety, suspicion, trigger history, and tolerance for environmental stimuli.
-
Assess immediate risk to self/others and need for rapid team activation.
-
If a client reports homicidal thoughts, assess target specificity, plan, means access, intent, and prior history of injuring others.
-
Assess client preferences for calming strategies during early distress.
-
Assess unit-level safety conditions (crowding, noise, staffing, escape routes).
-
Assess high-volatility clinical contexts (for example delirium, dementia, psychosis, intoxication/withdrawal, severe mental-illness exacerbation).
-
Assess for imminent-workplace-violence signs: confrontational behavior, angry demeanor, loud/aggressive or mumbling speech, threatening to leave, tense posturing, pacing, and aggressive acts.
-
Assess occupational-violence exposure and risk factors (for example isolated work settings, law-enforcement roles, alcohol-service environments, and healthcare roles).
-
In potentially combative encounters, assess hand behavior (for example fist clenching or gripping rails) as an early nonverbal tension signal.
-
Assess immediate and downstream abuse burden, including trauma symptoms, social withdrawal, and suicidal-ideation risk when severe or prolonged abuse is reported.
-
Assess for workplace incivility and horizontal/lateral violence signals (for example gossip, sabotage, exclusion, repeated disrespect) before escalation to overt aggression.
-
Assess workload-fatigue burden and its effect on situational awareness and response quality during potential violence events.
-
Assess nurse self-response signals (fight/flight activation, trauma-history sensitivity, and cultural-bias activation) that may alter communication or safety decisions.
-
Assess pediatric neglect cues such as poor hygiene, weather-inappropriate clothing, malnutrition/hunger, lack of supervision, and recurrent school absence.
-
Assess for pediatric physical-abuse red flags: patterned injuries, burns with clear demarcation, injury-history mismatch, delayed care seeking, and fear of caregivers.
-
Assess hidden injury risk in infants/toddlers, including possible abusive head trauma when behavior or neurologic status is inconsistent with reported mechanism.
-
Assess child sexual-abuse indicators such as genital pain/bleeding/discharge, difficulty sitting/walking, STIs, and age-incongruent sexualized behavior.
-
Assess emotional-abuse patterns including severe anxiety/depression, unusual aggression, withdrawal, self-denigration, and learning decline.
-
Assess adolescent dating-violence risk (including stalking) and ask direct, private relationship-safety questions when developmentally appropriate.
-
Assess bullying and cyberbullying exposure in children/adolescents, including school-avoidance behavior, social isolation, and abrupt academic decline.
-
Use normalizing language when screening bullying (for example asking whether the child has seen or experienced being picked on) to improve disclosure.
-
Assess elder-neglect indicators such as dehydration, malnutrition, poor hygiene, untreated medical/dental needs, or unsafe living conditions.
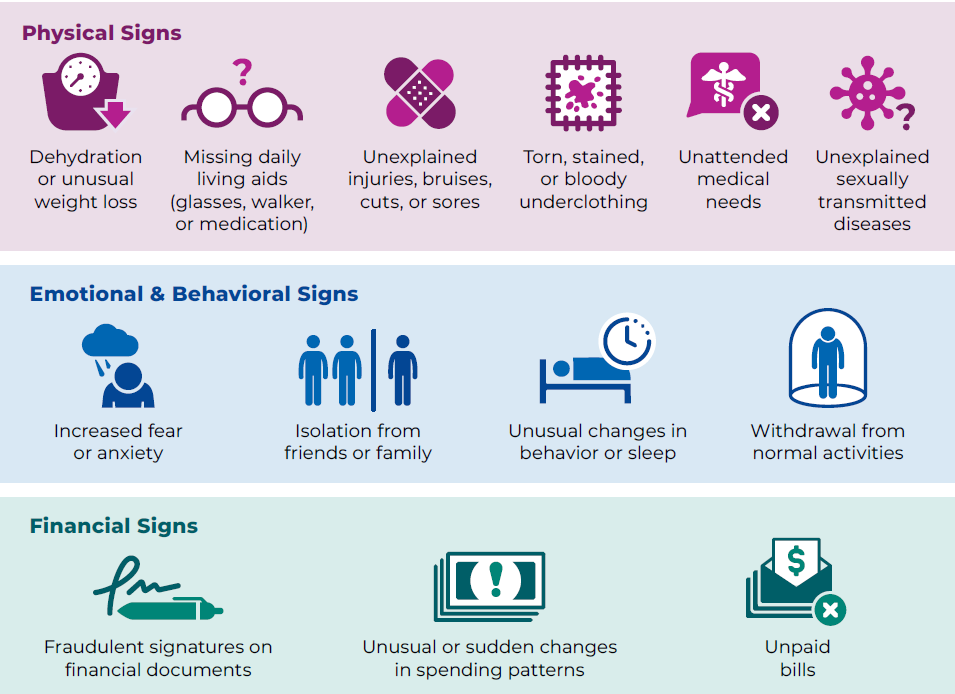 Illustration reference: OpenRN Nursing Health Promotion Ch.6.2.
Illustration reference: OpenRN Nursing Health Promotion Ch.6.2. -
In institutional elder-care settings, assess caregiver burnout, staffing shortages, and high workplace stress as abuse-risk multipliers.
-
Assess elder physical-abuse patterns that are inconsistent with accidental trauma, including maxillofacial injury, inner-arm or torso bruising, and recurrent injuries in different healing stages.
-
During elder-abuse screening, interview the older adult alone when feasible and use structured tools (for example EASI or H-S/EAST) as suspicion prompts rather than standalone diagnosis.
-
Document elder-abuse findings objectively with direct quotes and policy-concordant photo/environment evidence when permitted.
-
Assess downstream mental-health burden after violence exposure, including depression, anxiety, trauma symptoms, and suicidal ideation.
-
Assess risk of repeat victimization and possible victim-offender overlap when there is prior violence history.
-
Assess caregiver-child interaction patterns for fear-based control and account for possible caregiver victimization that can affect child safety.
Nursing Interventions
- Use calm, nonthreatening communication and collaborative de-escalation techniques.
- Use open, visible hands and a slight diagonal stance, and avoid blocking doorways during escalating encounters.
- Use nonprovocative stance and spacing: remain visible, avoid sudden approach or approaching from behind, and maintain about two arm-lengths with a clear exit path.
- In potentially escalating encounters, maintain door access and orientation to nearby exits/emergency call resources, especially when floating to unfamiliar areas.
- Reduce immediate triggers by moving cooperative agitated clients to a quiet, low-stimulation area when feasible.
- Apply least-restrictive alternatives first (redirection, time-out option, comfort, activity, reduced stimuli).
- Offer voluntary time-out as an immediate low-restriction option and clarify that the client may leave the area when ready.
- Use developmentally adapted behavior contracts (verbal or written) with clear expectations, reinforcement plan, and periodic review across care settings.
- Use collaborative-proactive problem solving to identify trigger patterns and agree on practical alternatives before escalation.
- When behavior is attention-seeking and not dangerous, use planned ignoring with immediate reinforcement of safe/on-task behavior.
- Use brief nonverbal signals or agreed gestures (for example eye contact cue or quiet-hand signal) to prompt self-control without public confrontation.
- Use limit-setting language rather than threats, and acknowledge emotions directly while asking clear safety questions (for example intent to harm self/others or weapon access).
- Remove neck-worn items (for example stethoscopes or badge lanyards) during escalating encounters to reduce strangulation risk.
- Use personal dress-for-safety practices (for example secure long hair, avoid pullable jewelry/scarves, and use breakaway lanyards).
- Offer PRN medication early when indicated and continue therapeutic presence after administration.
- Do not administer medication covertly or misrepresent the medication purpose; use transparent therapeutic communication.
- Use emergency medication without consent only for extreme immediate safety threat with provider/supervisory involvement and explicit documentation of information given and client response.
- Use seclusion/restraint only for emergency safety with required orders and continuous monitoring.
- If escalation continues despite verbal de-escalation, disengage safely and summon immediate team/security support per policy.
- If restrictive intervention appears likely, assign one staff leader for directions and pre-brief team roles before hands-on approach.
- When security staff are involved, keep client-care actions under nursing direction and use preplanned role clarity to reduce therapeutic conflict.
- Document violence-risk level and a collaborative intervention plan immediately, then notify provider/team for required legal and safety workflow.
- Conduct structured debriefing after incidents to support staff recovery, PTSD/burnout prevention, system learning, and client-perspective review.
- Participate in institutional violence-prevention training, threat reporting workflows, and cross-team response drills.
- Use formal behavioral-emergency activation pathways (for example BERT or equivalent team response) when available for timely multidisciplinary containment.
- Use violence-risk assessment tools at admission and repeat at defined intervals (often daily) to improve short-term prediction and team communication consistency.
- Reinforce a multifaceted workplace-violence strategy: prevention policy, staff training, communication de-escalation, and post-incident support access.
- In home-health or community travel settings, apply field-safety protocols: review violence-risk background information when available, use trained partner support for high-risk visits, carry charged communication devices, maintain location check-ins, and use prearranged emergency code words.
- In emergency settings, maintain a high index of suspicion for weapon access in actively violent clients and prioritize distance, exit access, and immediate team/security support.
- Activate mandated-reporting pathways and contact Child Protective Services (or equivalent agency) when child neglect/abuse is suspected per jurisdiction and policy.
- After child-abuse reporting, support trauma-informed follow-up pathways (for example child advocacy-center forensic interviewing, pediatric medical evaluation, and referral to trauma-focused psychotherapy such as TF-CBT).
- Coordinate multidisciplinary child-protection response (health care, mental health, social work, law enforcement, and education) and align plans with developmental stage and cultural context.
- Activate mandated-reporting pathways for suspected elder abuse/neglect and abuse of at-risk adults per jurisdiction and policy.
- Apply family-violence prevention across primary, secondary, and tertiary levels: strengthen social/economic supports, screen high-risk groups early, and coordinate shelter/protection resources after identified harm.
- For imminent community/social-violence risk, escalate to law enforcement or emergency pathways per policy while supporting immediate protective actions.
- Use context-matched screening tools (for example urgent danger tools for immediate IPV threat and ACE-focused tools for chronic trauma history) to guide follow-up planning.
- Provide age-appropriate prevention teaching on healthy relationships, consent, and stalking red flags for adolescents and caregivers.
- For school bullying plans, coach child/caregiver strategies: avoid known hotspots, move toward trusted adults, use calm assertive stop statements when safe, and coordinate with school/families for joint response planning.
- After disruptive incidents in youth settings, use simple restitution steps (for example repairing disorder or apologizing) to reinforce accountability and skills practice.
- Provide nonjudgmental counseling and resource linkage for high-risk populations, including veterans, pregnant patients, and patients with social-access barriers.
Restrictive Overuse Harm
Rapid escalation to seclusion/restraint without adequate less-restrictive attempts increases trauma and legal risk.
Pharmacology
PRN medication can prevent progression to violence when given at early agitation stages. Nursing responsibilities include informed explanation, monitoring effect trajectory, and documenting indication, response, and safety follow-up.
Clinical Judgment Application
Clinical Scenario
A client begins pacing, shouting, and clenching fists during visiting hours as noise levels rise on the unit.
- Recognize Cues: Escalation signs and environmental triggers are present.
- Analyze Cues: Progression to physical aggression is possible without immediate intervention.
- Prioritize Hypotheses: Priority is rapid de-escalation and stimulus reduction.
- Generate Solutions: Move to quiet area, validate distress, offer coping choice and PRN support.
- Take Action: Implement least-restrictive plan and activate team backup if risk increases.
- Evaluate Outcomes: Confirm de-escalation, update trigger-prevention plan, and debrief team.
Related Concepts
- anger-abuse-and-violence - Expands abuse cycle and aggression risk mechanisms.
- sexual-abuse-and-assault-care - Complements sexual-abuse response and trauma-informed follow-up care.
- restraints-and-restraint-alternatives - Details restrictive intervention hierarchy and safeguards.
- trauma-informed-care - Supports non-coercive, dignity-preserving safety practice.
- emergency-situations-and-rapid-response - Aligns escalation with urgent response workflows.
- client-engagement - Uses collaborative prevention plans to reduce recurrent incidents.