Delirium
Key Points
- Delirium is an acute, fluctuating confusional state that often signals serious underlying medical illness.
- Delirium affects millions of U.S. clients each year and is common in hospitalized older adults.
- Rapid identification and treatment of cause are critical to reduce morbidity and mortality.
- Delirium differs from dementia by sudden onset and variable attention/awareness changes.
- Nursing priorities include safety, reorientation support, family involvement, and prevention of complications.
- In end-of-life settings, delirium is highly prevalent and may improve when reversible contributors are identified early.
- Restraint avoidance and oversedation prevention are key because both can worsen delirium trajectory.
Pathophysiology
Delirium reflects acute brain dysfunction from systemic or neurologic disruption, commonly involving infection, metabolic imbalance, medication effects, intoxication/withdrawal, hypoxia, or postoperative stress.
Older adults and medically complex clients are at high risk, and untreated delirium can rapidly worsen outcomes.
In hospitalized older adults, delirium burden is high (including roughly one-third of hospitalized adults aged 70 years and older), with especially elevated rates after major surgery.
Temporary psychosis from medical causes can present with abrupt confusion, disorientation, agitation/combativeness, and hallucinations; this pattern should be treated as a possible life-threatening medical warning until reversible causes are addressed.
Classification
- Time course: Acute onset, fluctuating course.
- Subtype pattern: Hyperactive, hypoactive, or mixed delirium presentations.
- Cause pattern: Medical, toxicologic, withdrawal-related, or multifactorial etiologies.
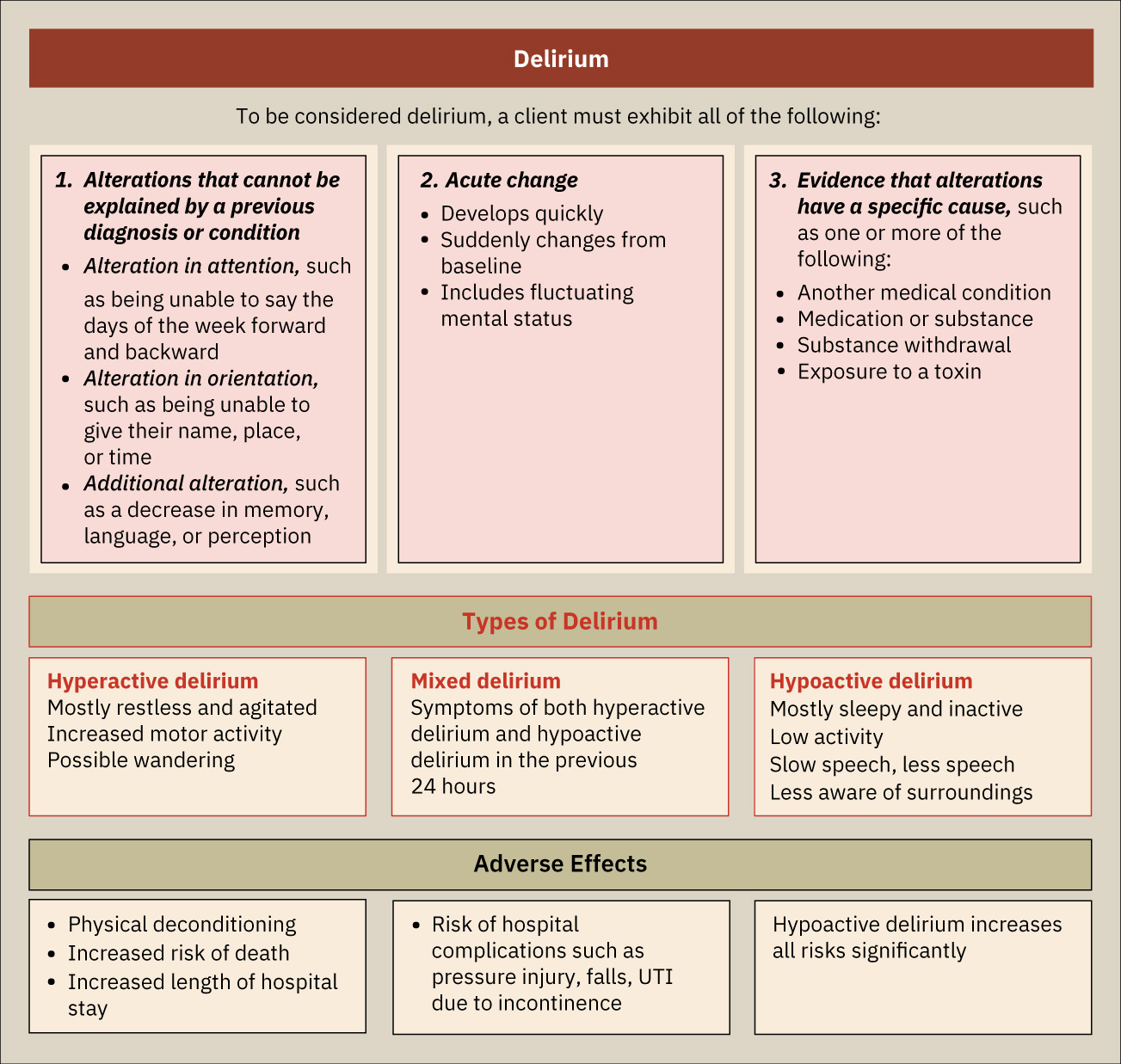 Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.24.4.
Illustration reference: OpenStax Psychiatric-Mental Health Nursing Ch.24.4.
Nursing Assessment
NCLEX Focus
New confusion in an older adult is delirium until proven otherwise.
- Assess onset pattern, attention changes, orientation, and fluctuation severity.
- Assess immediate medical contributors (infection, hypoxia, dehydration, electrolyte issues, medication change).
- Assess common precipitant clusters: dehydration/electrolyte imbalance, hospitalization (especially ICU-level stress), intoxication/withdrawal, kidney/liver failure, metabolic crises (for example DKA), severe pain, and sleep deprivation.
- Assess medication-related delirium risk across sedatives, opioids, anesthesia agents, antihistamines, anticholinergics, antidepressants, antipsychotics, and anticonvulsants.
- In older adults with sudden confusion, assess immediately for possible UTI and other occult infections; atypical UTI clues may include acute confusion, new incontinence, and shivering rather than dysuria.
- In palliative contexts, evaluate medication toxicity (including opioid toxicity) and metabolic insufficiency from organ failure as frequent causes.
- Assess safety risk for falls, aspiration, line removal, and agitation-related injury.
- Assess sleep disturbance, pain, sensory deficits, and environmental overstimulation.
- Assess family observations of baseline cognition versus acute changes.
- Screen with the Confusion Assessment Method (CAM) when available and escalate positive findings for urgent medical evaluation.
Nursing Interventions
- Escalate acute mental-status changes promptly for medical evaluation.
- Treat underlying causes while maintaining supportive, low-stimulation environment.
- Use frequent reorientation cues, hydration/nutrition support, and sleep hygiene strategies.
- Use visual orientation aids (for example whiteboards with date/time and team names) and keep caregiver assignments as consistent as possible to reduce disorientation.
- Involve familiar caregivers/family to reduce distress and improve cooperation.
- Use nonverbal pain-cue assessment (for example grimacing, guarding, posture change) when communication is impaired, and treat pain promptly.
- Remove avoidable barriers to family or designated surrogate presence according to client preferences.
- Provide orientation supports such as visible clocks/calendars and keep glasses/hearing aids in use to reduce sensory mismatch.
- Encourage early mobilization when safe and prevent prolonged bedrest deconditioning.
- Use supportive nonpharmacologic calming measures (for example gentle touch/massage, distraction, relaxation cues) with family-assisted reorientation when tolerated.
- Avoid restraints whenever possible and use the least-restrictive safety approach.
- Monitor closely for deterioration, withdrawal syndromes, and complication risk.
Sedation-First Pitfall
Sedating without cause-focused evaluation can mask worsening physiology and delay life-saving treatment.
Pharmacology
Pharmacologic decisions target underlying cause and severe agitation only when necessary for safety. Plans may include carefully titrated neuroleptic options (for example haloperidol or chlorpromazine) and selected benzodiazepine use while nursing care emphasizes cautious monitoring for adverse effects and frequent reassessment of need. Oversedation can worsen delirium and should be actively avoided.
Clinical Judgment Application
Clinical Scenario
A hospitalized older adult becomes abruptly disoriented overnight, pulls at lines, and alternates between agitation and drowsiness.
- Recognize Cues: Sudden fluctuating cognition suggests delirium.
- Analyze Cues: Immediate medical causes are likely and potentially reversible.
- Prioritize Hypotheses: Priority is urgent medical workup plus injury prevention.
- Generate Solutions: Activate delirium protocol, review medications, and reduce environmental triggers.
- Take Action: Implement safety supports and coordinate rapid diagnostics/treatment.
- Evaluate Outcomes: Reassess cognition trend, cause correction, and complication prevention.
Related Concepts
- mild-neurocognitive-disorders - Differentiates gradual mild decline from acute delirium.
- dementia - Contrasts chronic progressive patterns with delirium fluctuations.
- emergency-situations-and-rapid-response - Guides urgent escalation pathways.
- violence-and-safety - Supports safe management of agitation and confusion.
- nursing-assessment-and-clinical-tools - Reinforces structured acute-status assessment.