Shock Overview
Key Points
- Shock is a state of inadequate cellular/tissue perfusion that threatens organ function and survival.
- Early shock activates sympathetic compensation (vasoconstriction, tachycardia, stress-hormone release), but persistent hypoperfusion leads to tissue hypoxia and cell death.
- Types include cardiogenic, hypovolemic, septic, and neurogenic pathways, each with different causes but a shared endpoint of perfusion failure.
- Early recognition and intervention are critical before progression to irreversible stages.
Pathophysiology
Adequate perfusion requires coordinated cardiovascular pump function, vascular tone, oxygen delivery, and end-organ regulation. In shock, circulatory dysfunction reduces tissue oxygen delivery. Cardiac output (CO = stroke volume x heart rate) is especially vulnerable when preload, afterload, or contractility becomes unfavorable. Compensatory sympathetic activation increases catecholamines and cortisol, driving:
- Increased heart rate
- Peripheral vasoconstriction
- Temporary blood-pressure support
- Increased circulating glucose for stress-energy demand
When compensation fails, tissue oxygen debt rises, anaerobic metabolism increases, and lactic acid accumulates. Persistent severe tachycardia can eventually reduce ventricular filling and worsen effective output. Ongoing hypoperfusion leads to organ dysfunction and eventual cell death.
Hemodynamic Monitoring
Hemodynamic monitoring helps evaluate perfusion status and response to therapy.
| Parameter | Typical reference | Shock pattern |
|---|---|---|
| Cardiac output (CO) | About 4-8 L/min | Decreased in low-output states |
| Cardiac index (CI) | About 2.5-4.0 L/min/m² | Often reduced when perfusion is inadequate |
| Stroke volume (SV) | About 60-100 mL/beat | Often reduced in pump-failure or preload-deficit states |
| Mean arterial pressure (MAP) | About 70-100 mmHg | Decreased; perfusion concern when <65 mmHg |
| Central venous pressure (CVP) | About 2-6 mmHg | Often decreased in volume-loss states; may rise in selected obstructive/cardiogenic states |
| Pulmonary artery pressure (PAP) | About 11-20 mmHg (rest) | Can rise with pulmonary vascular or left-sided cardiac dysfunction |
| Pulmonary artery occlusion pressure (PAOP/wedge) | About 8-12 mmHg | May increase in left-sided filling-pressure overload |
| Systemic vascular resistance (SVR) | About 800-1200 dynes/sec/cm⁻⁵ | Low in distributive states and high in vasoconstrictive states |
- Noninvasive assessment: pulse, blood pressure, capillary refill, skin temperature, edema pattern.
- Invasive assessment: arterial-line MAP and central-access pressure monitoring when continuous high-acuity trends are required.
- Advanced invasive assessment in selected ICU patients may include pulmonary-artery-catheter data to refine low-output versus vasomotor shock interpretation.
- Interpret hemodynamic variables as a profile (pump, preload, and afterload) rather than isolated numbers.
Stages of Shock
Initial Stage
- Cellular perfusion begins to decline.
- SNS activation starts, but overt clinical findings can be subtle.
- Typical early cues: mild agitation, slight urine-output decline, and normal-to-slightly elevated vital signs.
Compensatory Stage
- Blood pressure begins to fall and compensatory reflexes intensify.
- Baroreceptor-mediated sympathetic drive attempts to maintain perfusion pressure.
- Catecholamine surge (norepinephrine/epinephrine) increases vascular tone and heart rate; blood flow is redistributed to brain and heart.
- RAAS activation increases sodium-water retention and vasoconstriction, providing temporary blood-pressure support.
- Clinical deterioration becomes more apparent if perfusion is not restored.
- Common compensatory-stage findings: low blood pressure, tachycardia, cool skin, decreased urine output, and normal-to-slightly elevated respiratory rate.
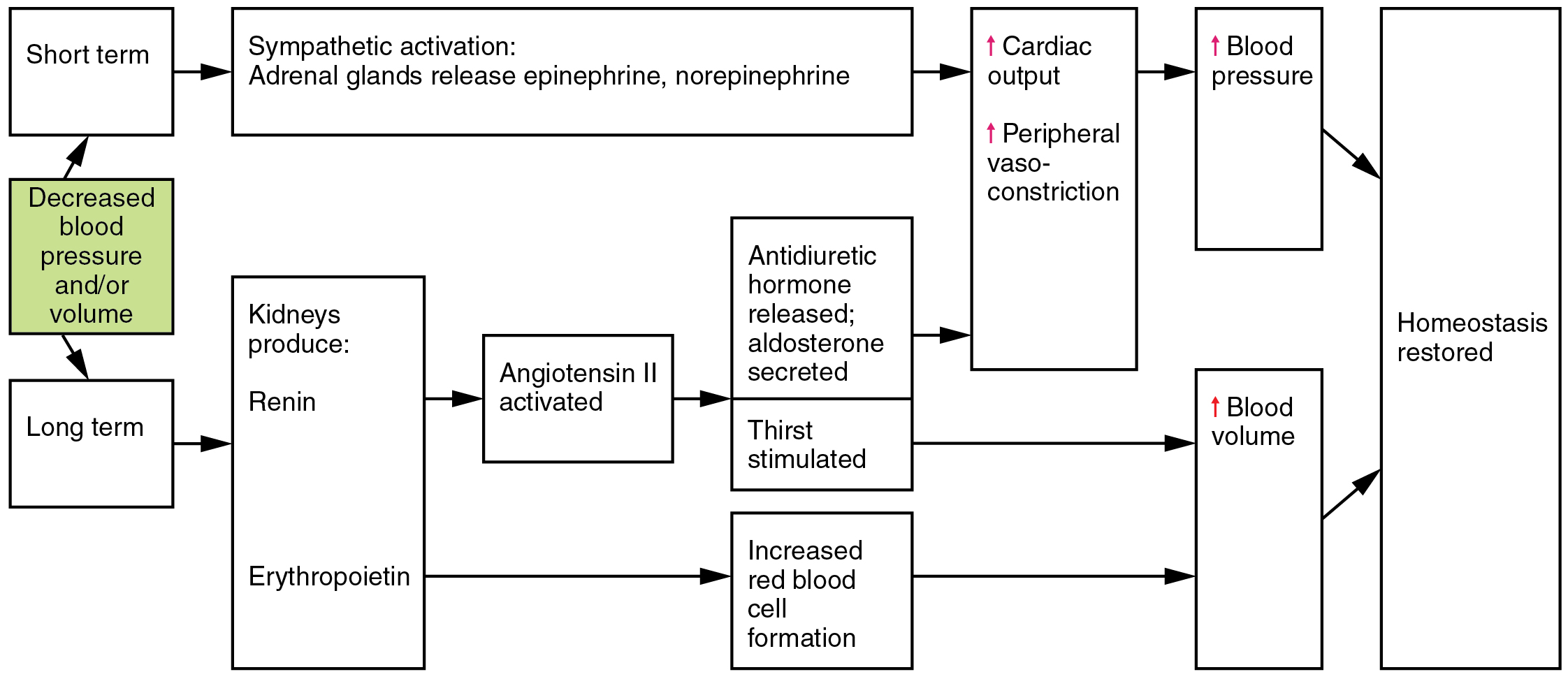 Illustration reference: OpenRN Health Alterations Ch.5.2.
Illustration reference: OpenRN Health Alterations Ch.5.2.
Early Organ-Level Consequences During Compensation
- Renal hypoperfusion drives renin release and fluid-conserving endocrine response.
- Ongoing pulmonary endothelial injury can increase alveolar-capillary permeability, causing pulmonary edema.
- Respiratory compromise may progress to acute respiratory distress syndrome (ARDS) in severe/decompensating pathways.
Progressive Stage
- Cellular perfusion drops further and capillary permeability rises markedly.
- Protein and fluid leak from intravascular space into interstitial space, worsening effective circulating volume.
- This capillary-leak pattern accelerates tissue hypoperfusion and promotes multi-organ dysfunction progression.
- Typical progressive-stage cues include worsening hypotension/tachycardia/tachypnea, cool clammy skin, weak distal pulses, and urine output decline.
- Ongoing hypoxia can drive metabolic acidosis and dysrhythmia/ischemic cardiac complications.
Refractory Stage
- Profound hypotension and cellular failure persist despite treatment.
- Anaerobic metabolism, lactic acidosis, and severe capillary leak continue with limited reversibility.
- Findings often include mottled skin, near-anuric urine output, weak-to-absent peripheral pulses, and severe end-organ failure.
Organ-System Deterioration Pattern in Progressive/Refractory Shock
- Cardiovascular: tachydysrhythmias, myocardial ischemia/infarction, circulatory collapse risk.
- Pulmonary: pulmonary edema, impaired gas exchange, rising work of breathing, ARDS progression.
- Neurologic: altered level of consciousness from cerebral hypoperfusion.
- Renal: urine output frequently below 30 mL/hour with rising BUN/creatinine.
- Gastrointestinal/hepatic: barrier injury, poor nutrient absorption, jaundice, rising liver-injury markers.
- Vascular/skin: third spacing, peripheral edema, pallor or cool clammy/mottled skin.
- Metabolic: electrolyte imbalance and metabolic acidosis.
Stage-Based Vital Sign Pattern
| Stage | Blood pressure | Heart rate | Respiratory rate | Urine output | Temperature | Skin/pulses |
|---|---|---|---|---|---|---|
| Initial | Normal to slightly high | Normal to slightly high | Often near normal | Mild decline possible | Usually normal | Early perfusion change may be subtle |
| Compensatory | Low | Elevated | Normal to mildly elevated | Decreased | Usually normal | Cool skin, perfusion redistribution |
| Progressive | Low | Elevated | Elevated | Low | Often low | Cool clammy skin, weak distal pulses |
| Refractory | Persistently low despite treatment | Markedly elevated | Elevated | Low to near zero | Low | Mottled cool skin, weak/absent peripheral pulses |
Multiorgan Dysfunction Risk
Prolonged shock can progress to multiorgan dysfunction syndrome (MODS). Risk is higher in older adults and patients with multiple comorbidities, especially in severe hypovolemic or septic pathways.
Nursing Assessment
- Track mental-status changes, urine output, skin perfusion cues, and vital-sign trends.
- Interpret blood pressure with perfusion context; prioritize MAP trend over isolated single values.
- Identify early progression from subtle compensation to decompensation.
- Escalate rapidly for persistent hypotension, worsening perfusion, or rising organ-dysfunction indicators.
Nursing Interventions
- Support rapid cause-directed stabilization per protocol and provider orders.
- Ensure frequent reassessment of perfusion indicators and hemodynamic trends.
- Coordinate oxygenation, fluid, and vasoactive-therapy readiness in high-risk patients.
- In refractory low-output cardiogenic pathways, anticipate temporary mechanical-circulatory support escalation (for example intra-aortic-balloon-pump counterpulsation) with strict bleeding and distal neurovascular checks.
- In refractory cardiopulmonary failure, prepare for extracorporeal-membrane-oxygenation escalation and monitor major complication domains (bleeding, thrombosis, infection, and limb ischemia) with interdisciplinary coordination.
- Communicate trend deterioration early to prevent progression to irreversible shock stages.
Clinical Judgment Application
Clinical Scenario
A patient develops rising heart rate, new agitation, cool extremities, and MAP trending from 74 to 66 mmHg over 1 hour.
- Recognize Cues: Tachycardia, mental-status change, cool skin, falling MAP.
- Analyze Cues: Compensatory physiology is failing to maintain adequate tissue perfusion.
- Prioritize Hypotheses: Impending progression of shock is the immediate threat.
- Generate Solutions: Escalate monitoring intensity, prepare rapid stabilization orders, and reassess perfusion targets.
- Take Action: Activate high-acuity response workflow, obtain serial perfusion data, and support ordered interventions.
- Evaluate Outcomes: MAP and urine output improve, mental status stabilizes, and end-organ perfusion signs recover.
Related Concepts
- hypovolemic-shock - Volume-loss shock pathway with source-control and rapid-resuscitation priorities.
- cardiogenic-shock - Low-output pump-failure phenotype with vasoactive and mechanical-support escalation needs.
- sepsis - Septic pathways can progress to distributive shock and multi-organ dysfunction.
- cardiovascular-system - Pump function and vascular tone are central shock determinants.
- vital-sign-indicators-of-physiologic-functioning-and-homeostasis - Trend interpretation is essential in early shock recognition.
- cvad-indications-and-device-selection - Central access supports invasive hemodynamic monitoring in unstable states.
Self-Check
- Why can MAP be more useful than isolated systolic pressure in shock monitoring?
- Which early cues suggest transition from initial to compensatory shock?
- What trend pattern should trigger immediate escalation even before severe hypotension appears?