CVAD Indications and Device Selection
Key Points
- CVAD placement is commonly indicated for long-term infusion therapy, high-osmolarity infusions, vesicant medications, and selected emergency access needs.
- Central infusion through a large vein (such as the superior vena cava) reduces irritation risk by hemodilution.
- Device and site selection should be individualized by therapy duration, medication profile, vascular characteristics, and patient-specific risk factors.
- PICC lines are not ideal for all clients; for example, vein-preservation priorities in end-stage renal disease can favor alternate access planning.
- CVAD insertion requires specially trained clinicians, while bedside nursing maintenance and aseptic care are ongoing safety priorities.
- CVAD insertion is invasive and risk-bearing, so alternative access should be considered before placement when appropriate.
Pathophysiology
CVAD use is driven by vascular safety and delivery reliability. High-osmolarity solutions (for example, total parenteral nutrition and hypertonic IV fluids) and vesicants can injure peripheral vessels or surrounding tissue if infiltration or extravasation occurs. Delivering these therapies into a large central vein improves dilution and reduces local endothelial injury risk.
Common insertion pathways include neck, chest, or groin venous entry (for example internal jugular, subclavian, or femoral) with catheter advancement until the tip resides centrally (such as superior vena cava, inferior vena cava, or right atrial region per device purpose and policy).
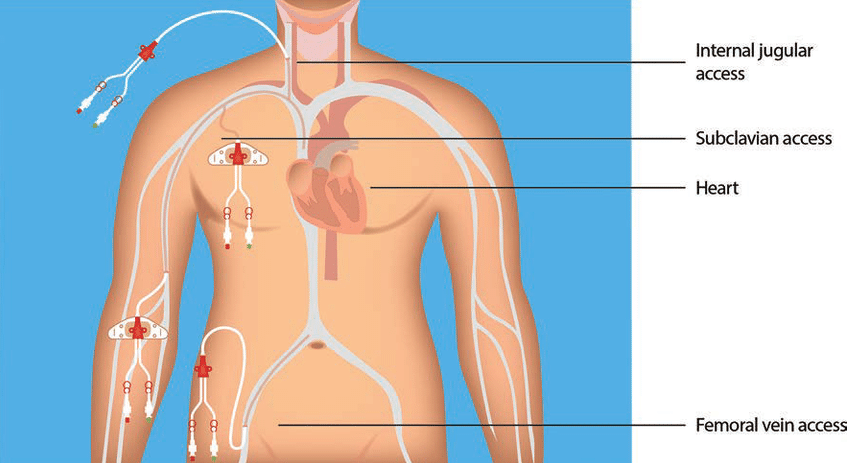 Illustration reference: OpenRN Nursing Advanced Skills Ch.4.1.
Illustration reference: OpenRN Nursing Advanced Skills Ch.4.1.
For critically ill patients, central access can also support rapid fluid resuscitation and hemodynamic monitoring. In this context, central venous pressure reflects pressure near right atrial entry and can be used as a preload-oriented volume-status measure during resuscitation planning.
Classification
- PICC: Thin catheter inserted through an upper-arm vein and advanced to the superior vena cava; commonly used for weeks to months and may be used for blood sampling per policy. Use caution in clients with end-stage renal disease, thrombosis history, or hypercoagulable risk when long-term vein preservation is needed.
- Non-tunneled CVAD: Typical duration days to several weeks; used for shorter high-acuity needs. In adults, subclavian placement is often preferred over femoral access when clinically feasible because thrombosis and infection risk may be lower.
- External tunneled CVAD: Long-term or permanent access with a subcutaneous tunnel to reduce bloodstream entry risk.
- Implanted venous access device (port/IVAD): Long-term or permanent access attached to a reservoir pocket and accessed with a noncoring needle; often less visible and lower-maintenance in daily activity than external devices.
- Lumen configuration: Single-, double-, or multi-lumen configurations are selected by therapy needs. Typical triple-lumen use patterns place fluids/TPN/medications in proximal or middle lumens, while a larger distal lumen is commonly reserved for blood administration, blood sampling, and central venous pressure monitoring per policy.
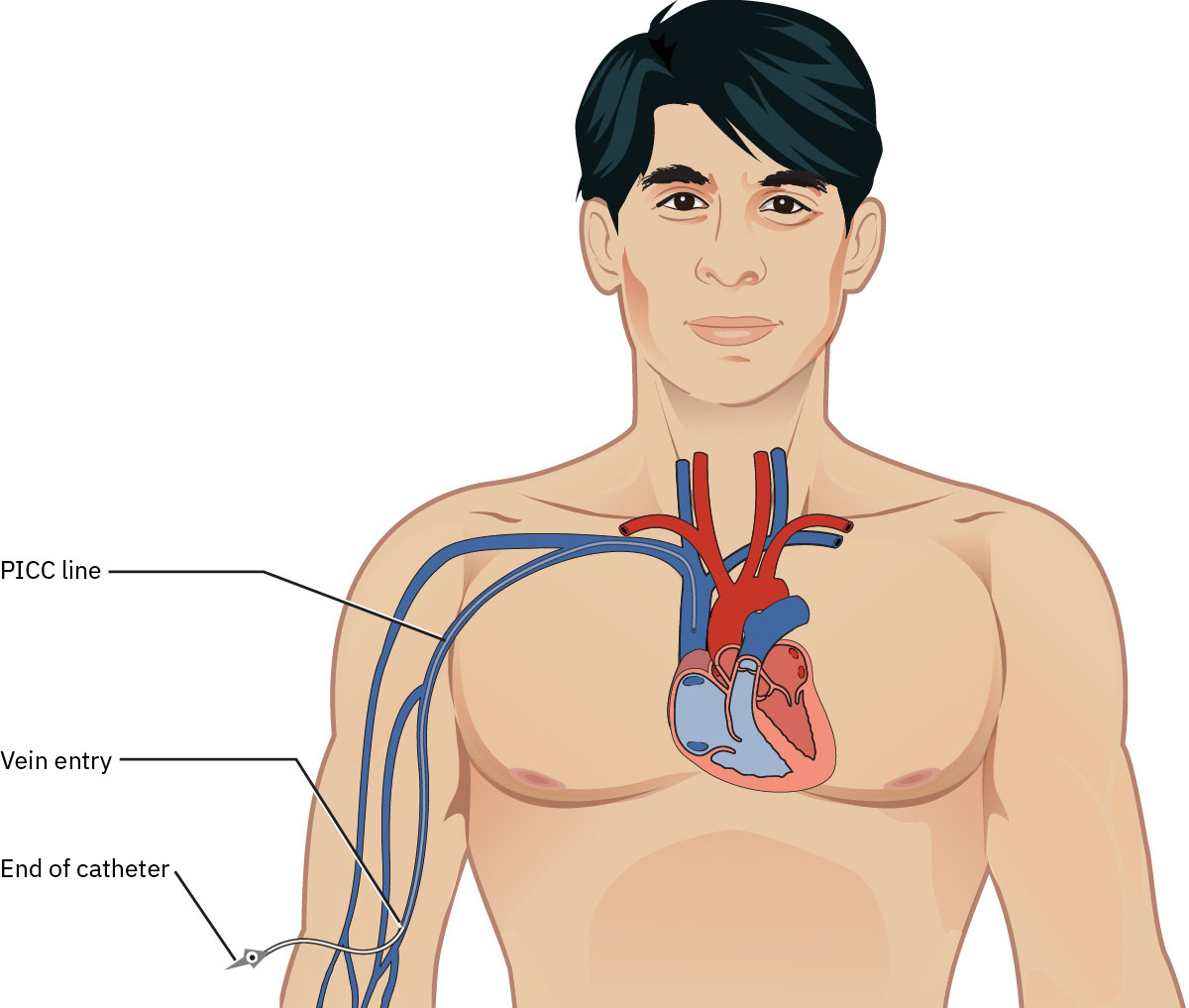 Illustration reference: OpenStax Clinical Nursing Skills Ch.13.
Illustration reference: OpenStax Clinical Nursing Skills Ch.13.
Nursing Assessment
NCLEX Focus
Prioritization questions often ask which infusion types require central access and which patient factors make a specific device safer.
- Assess indication type: long-duration therapy, vesicant administration, high-osmolarity infusion, or resuscitation need.
- Assess expected duration of therapy before recommending device type.
- Assess expected lumen needs before insertion (for example separate lumen use for blood products, CVP monitoring, parenteral nutrition, and incompatible medications).
- Assess vessel characteristics, prior infusion history, medical history, age, and cognitive factors relevant to maintenance safety.
- Assess whether ultrasound-guided insertion support is available because this improves insertion success and can reduce placement complications.
- Assess contraindication risk patterns, including peripheral-flow limitations or thrombosis-prone history.
Nursing Interventions
- Collaborate with provider and care team on device/site planning before insertion.
- Verify that indication, risk explanation, and informed plan are documented in the medical record.
- Support site-appropriate safety strategy (central vs peripheral approach) based on therapy profile.
- Verify catheter-tip location by accepted method (for example real-time fluoroscopy or post-procedure chest X-ray when fluoroscopy is not used) and ensure tip location documentation is present before ongoing use.
- Stabilize the catheter with sutured or sutureless engineered securement per device type and policy to reduce dislodgement and treatment interruption.
- Reinforce strict aseptic practice during insertion support and all maintenance tasks because CVADs increase bloodstream-infection risk.
- Perform structured surveillance for thrombosis, occlusion, phlebitis, and skin or tissue injury.
Extravasation Injury Risk
Vesicant leakage into surrounding tissue can cause severe tissue injury or destruction and requires immediate escalation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| breast-cancer-chemotherapy-safety-and-support (antineoplastics) | Vesicant chemotherapy agents | Prefer central delivery when vesicant risk is significant to reduce severe local injury potential. |
| antibiotics | Selected IV antibiotics with vessel-irritating profiles | Route and device choice should consider endothelial irritation risk and treatment duration. |
| vasopressors | Continuous vasopressor infusions | Central administration is commonly preferred for high-risk extravasation prevention. |
Clinical Judgment Application
Clinical Scenario
A patient requires prolonged infusion of hypertonic nutrition and intermittent vesicant medications, with limited peripheral vein quality.
- Recognize Cues: High-osmolarity and vesicant therapies with expected long treatment course.
- Analyze Cues: Peripheral access increases risk of phlebitis, thrombosis, and tissue injury if dislodgement occurs.
- Prioritize Hypotheses: Primary priority is selecting the safest durable access route.
- Generate Solutions: Compare PICC, tunneled CVAD, and implanted port based on duration and patient factors.
- Take Action: Implement team-selected CVAD plan and begin ongoing complication monitoring.
- Evaluate Outcomes: Therapy proceeds with reliable access and no major catheter-related harm.
Related Concepts
- peripheral-iv-access - Peripheral routes may be insufficient for vesicants or prolonged high-osmolarity therapy.
- parenteral-nutrition-monitoring - Total parenteral nutrition commonly requires central access planning.
- clabsi-prevention-bundle-implementation - Infection prevention is essential after central-line placement.
- blood-transfusion-verification-initiation-and-reaction-response - Another high-risk intravascular workflow requiring strict verification practice.
- intravenous-medication-administration-safety - Shared infusion-safety principles for route validation and reassessment.
Self-Check
- Why are high-osmolarity and vesicant infusions often routed through central veins rather than peripheral veins?
- Which factors should guide selection between PICC, non-tunneled CVAD, tunneled CVAD, and implanted port?
- What immediate nursing action is required when extravasation of a vesicant is suspected?