Placenta Previa
Key Points
- Placenta previa is placental implantation in the lower uterus near or covering the internal cervical os.
- Classic bleeding pattern is bright red vaginal bleeding with or without pain.
- Major risks include maternal hemorrhage, preterm birth, and urgent operative-delivery needs.
- Digital vaginal examination is avoided when placenta previa is suspected or confirmed because it can trigger severe bleeding.
- Partial and complete os coverage generally require cesarean delivery.
Pathophysiology
In placenta previa, placental tissue occupies the lower uterine segment rather than the usual fundal location. As the lower uterine segment stretches in later pregnancy, placental-edge disruption can occur and cause recurrent or sudden bleeding.
Hemorrhage risk can escalate rapidly during pregnancy or labor. When os coverage is partial or complete, cervical dilation and labor increase risk of placental tearing and catastrophic maternal-fetal blood loss.
Classification
- Low-lying placenta: Placental edge is near the internal os but does not completely cover it.
- Partial previa: Placenta partially covers the internal cervical os.
- Complete previa: Placenta fully covers the internal cervical os.
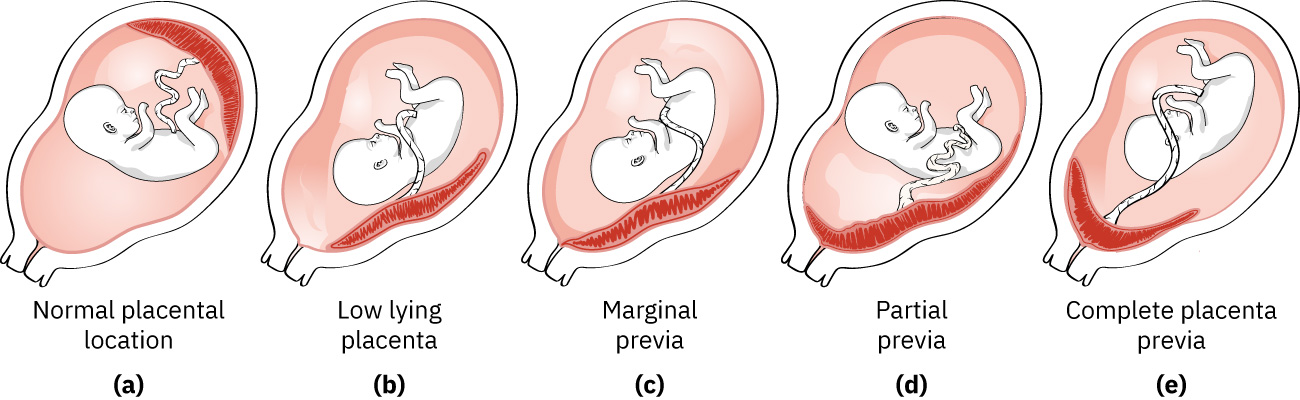 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.12.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.12.2.
Nursing Assessment
NCLEX Focus
Painless bright red bleeding in later pregnancy should trigger immediate placenta-previa safety precautions until ruled out.
- Assess bleeding quantity, color, recurrence pattern, and associated symptoms.
- Assess maternal hemodynamics and shock indicators with trend-based vital monitoring.
- Monitor fetal status continuously when active bleeding is present.
- Review risk factors including prior previa, multiparity, multifetal gestation, prior uterine surgery/cesarean birth, advanced maternal age, assisted reproduction, and smoking.
- Confirm placenta location by ultrasound and avoid digital cervical examination.
Nursing Interventions
- Activate antepartum-bleeding protocol and prioritize maternal-fetal stabilization.
- Enforce no-digital-vaginal-exam precautions until placenta location is confirmed safe.
- Prepare blood-product and surgical readiness if bleeding escalates.
- Reinforce pelvic-rest/activity-restriction orders when prescribed.
- Provide anticipatory teaching on cesarean planning when os coverage is partial or complete.
- Teach urgent return precautions for any recurrent bleeding, pain, dizziness, or reduced fetal movement.
Exam-Triggered Hemorrhage Risk
Digital cervical examination in undiagnosed placenta previa can precipitate severe placental bleeding and rapid decompensation.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| blood-transfusion-verification-initiation-and-reaction-response (blood-products) | PRBC/plasma/platelet support contexts | Prepare early in active hemorrhage or hemodynamic instability. |
| corticosteroids (antenatal-corticosteroids) | preterm-delivery-risk contexts | Used when early delivery risk is elevated to support fetal lung maturity. |
Clinical Judgment Application
Clinical Scenario
A 32-week patient presents with sudden painless bright red vaginal bleeding; ultrasound shows placental edge crossing the internal os.
- Recognize Cues: Antepartum bright red bleeding with confirmed os coverage.
- Analyze Cues: Findings are consistent with placenta previa and high hemorrhage risk.
- Prioritize Hypotheses: Immediate priority is maternal-fetal stabilization and hemorrhage prevention.
- Generate Solutions: Initiate continuous monitoring, bleeding protocol, and cesarean-readiness planning.
- Take Action: Maintain no-vaginal-exam precautions and coordinate multidisciplinary obstetric response.
- Evaluate Outcomes: Bleeding is stabilized and delivery plan is safely aligned with previa severity.
Related Concepts
- conditions-limited-to-pregnancy - Placenta previa is a major pregnancy-specific bleeding disorder.
- placental-abruption - Critical antepartum-bleeding differential with different pain/bleeding pattern.
- obstetrical-conditions-affecting-labor-and-birth - Placental-location disorders alter intrapartum management pathways.
- cesarean-section - Definitive delivery route in partial/complete previa pathways.
Self-Check
- Which bleeding pattern is most characteristic of placenta previa?
- Why are digital vaginal exams avoided in suspected placenta previa?
- How does previa severity change delivery-planning decisions?