Fetal Heart Rate and Contraction Patterns
Key Points
- Normal fetal heart rate baseline is 110 to 160 bpm measured over a 10-minute segment.
- Moderate variability (6 to 25 bpm) is the most reassuring variability pattern.
- Deceleration type and timing guide urgency: early is usually benign, while late, repetitive variable, and prolonged patterns increase hypoxia concern.
- Uterine tachysystole and Category II to III tracing progression require rapid reassessment and escalation.
Pathophysiology
Fetal heart rate (FHR) reflects dynamic autonomic regulation and oxygenation status during labor. Sympathetic input tends to increase FHR, while parasympathetic input decreases it; changes in oxygenation and acid-base status alter this balance and produce recognizable tracing patterns. Beat-to-beat variability is a key marker of intact fetal CNS-autonomic responsiveness; moderate variability usually aligns with better oxygenation and acid-base status.
Uterine contractions can transiently affect placental and cord blood flow. Pattern interpretation therefore relies on integrating baseline rate, variability quality, periodic accelerations/decelerations, and contraction context rather than any single tracing feature.
Classification
- Baseline: Average FHR in 10 minutes, excluding major periodic changes and marked variability, and typically documented in 5-bpm increments; tachycardia is more than 160 bpm for 10 minutes and bradycardia is less than 110 bpm for 10 minutes.
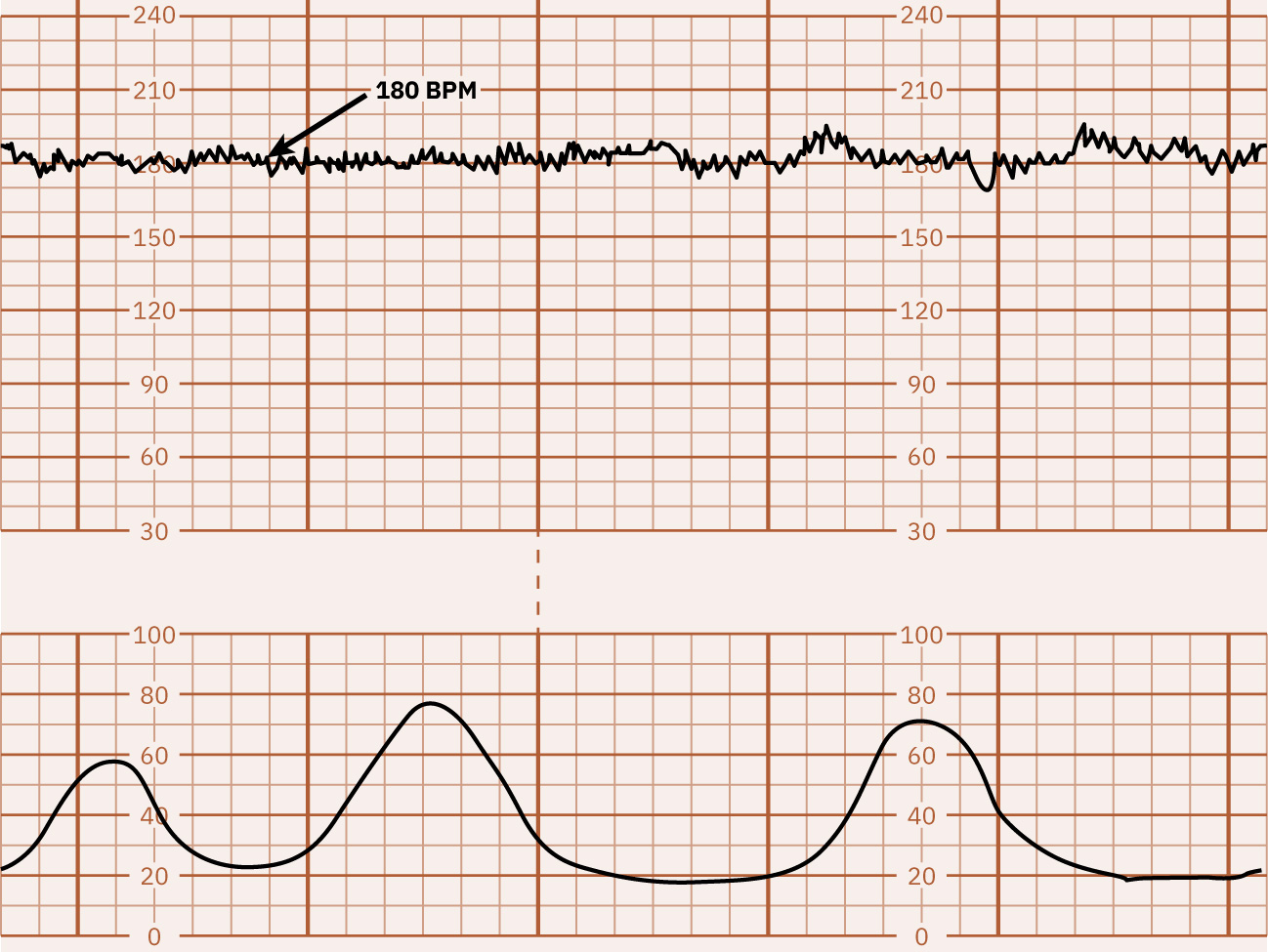 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
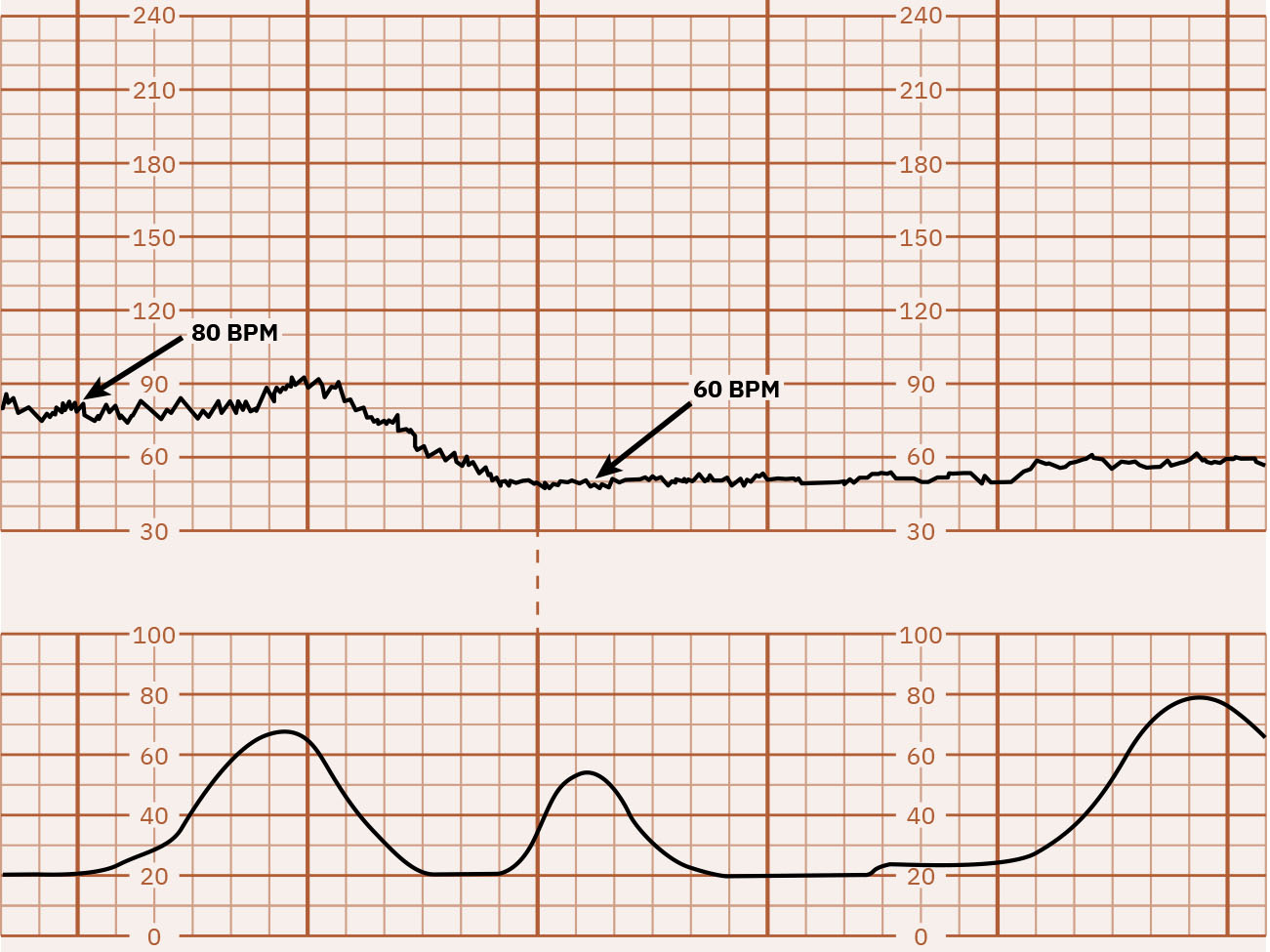 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
- Variability: Minimal (5 bpm or less), moderate (6 to 25 bpm, reassuring), marked (more than 25 bpm), or absent; sinusoidal pattern is a separate high-risk waveform (typically smooth regular 3 to 5 cycles per minute) with absent true variability. Minimal variability may indicate acidemia risk but must be interpreted with full clinical context rather than as a single definitive marker, while absent variability is strongly concerning for severe compromise/metabolic acidosis until reversible causes are excluded. Marked variability can make baseline determination difficult and may accompany second-stage hypoxia-related stress.
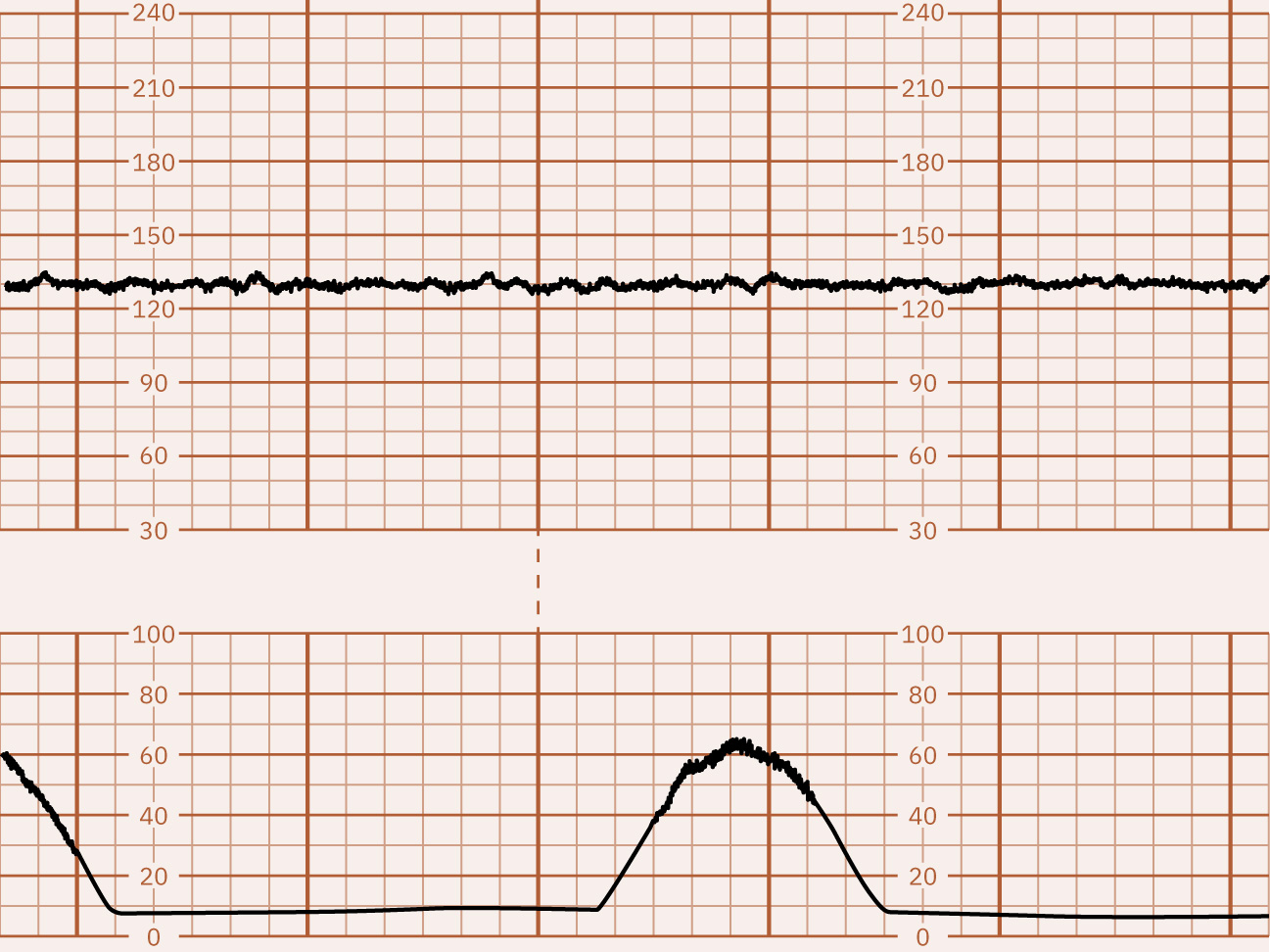 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
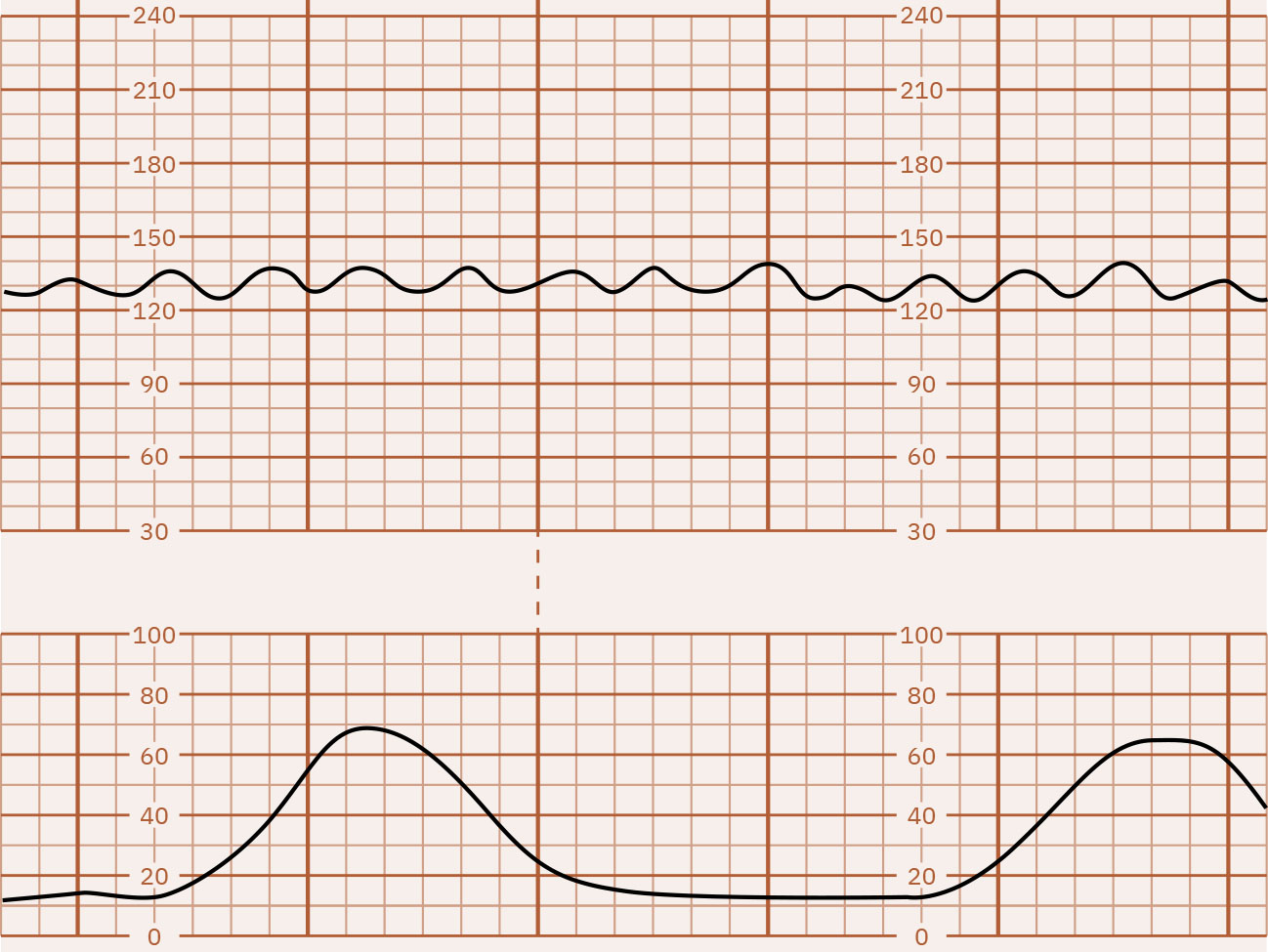 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
- Periodic increases: Accelerations are abrupt rises with onset-to-peak less than 30 seconds; at or beyond 32 weeks they are at least 15 bpm above baseline for at least 15 seconds and less than 2 minutes, while before 32 weeks a 10-by-10 pattern is expected. Accelerations are generally reassuring signs of fetal well-being.
- Periodic decreases: Early decelerations are gradual mirror patterns (typically head-compression vagal response and often benign), late decelerations begin with contractions but recover after contraction completion with nadir after the contraction peak, variable decelerations are abrupt drops (often 15 bpm or more below baseline for at least 15 seconds) from cord-compression mechanisms that may or may not align with contractions, and prolonged decelerations are isolated drops (at least 15 bpm) lasting 2 to 10 minutes.
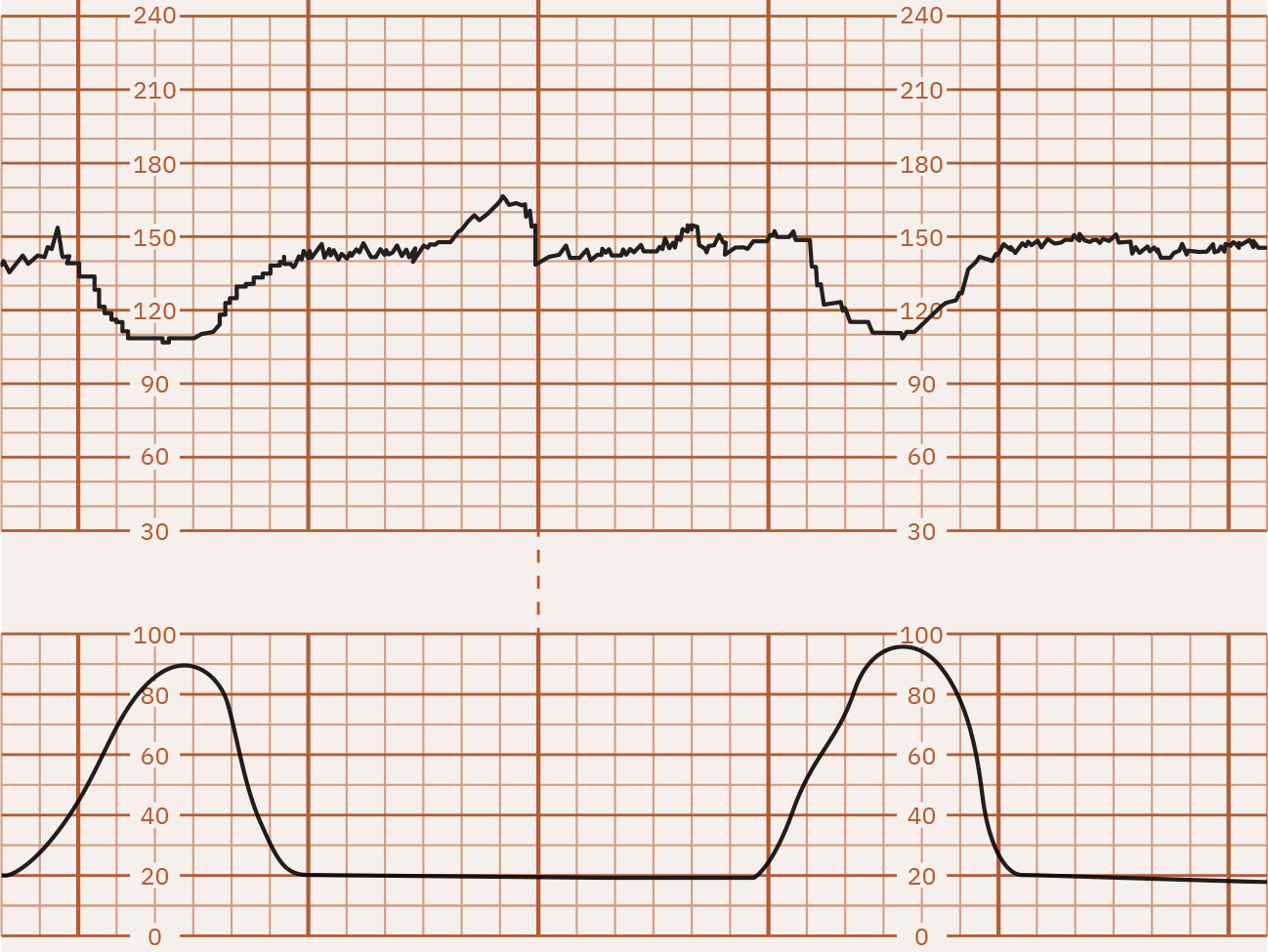 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
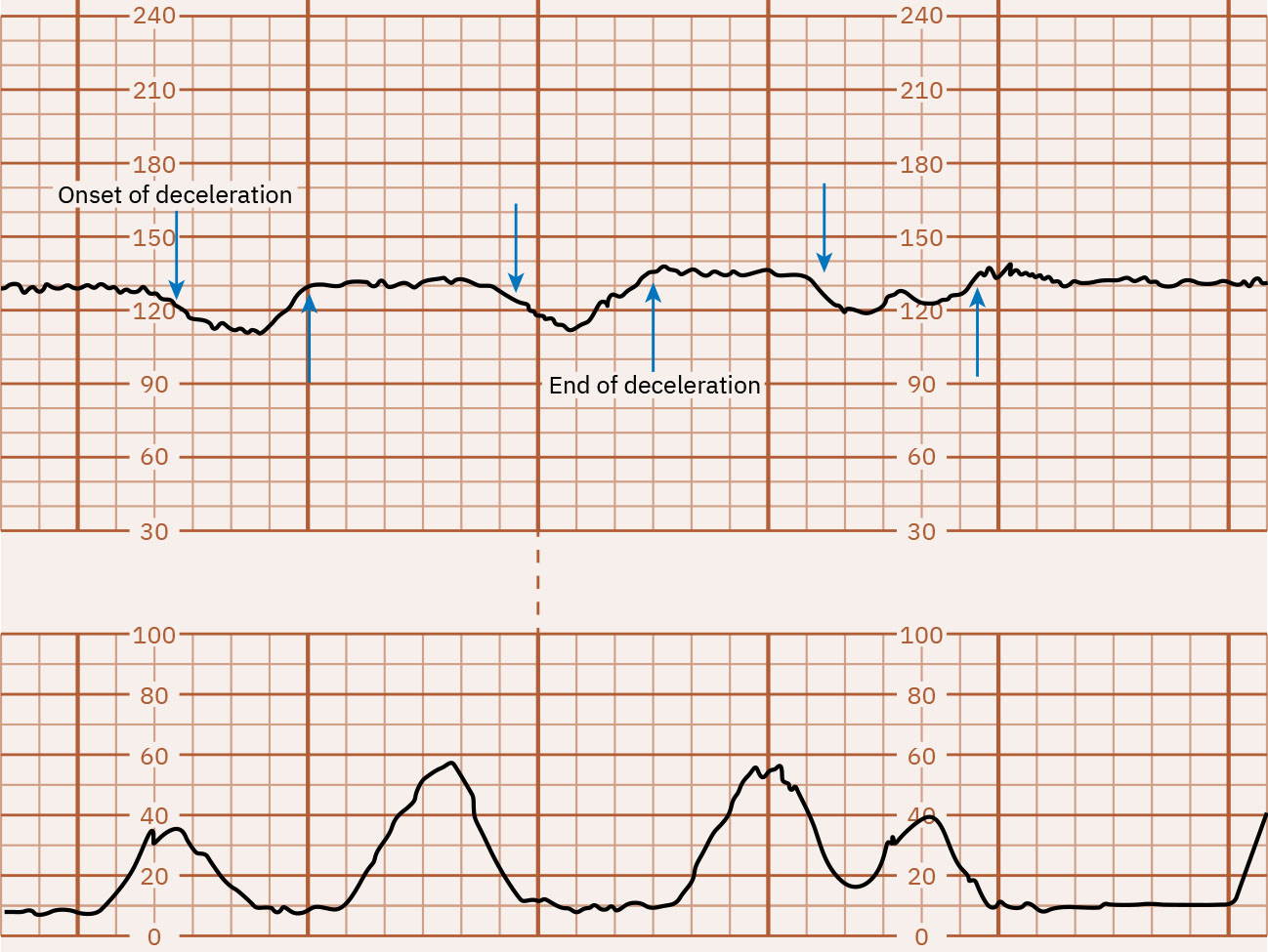 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
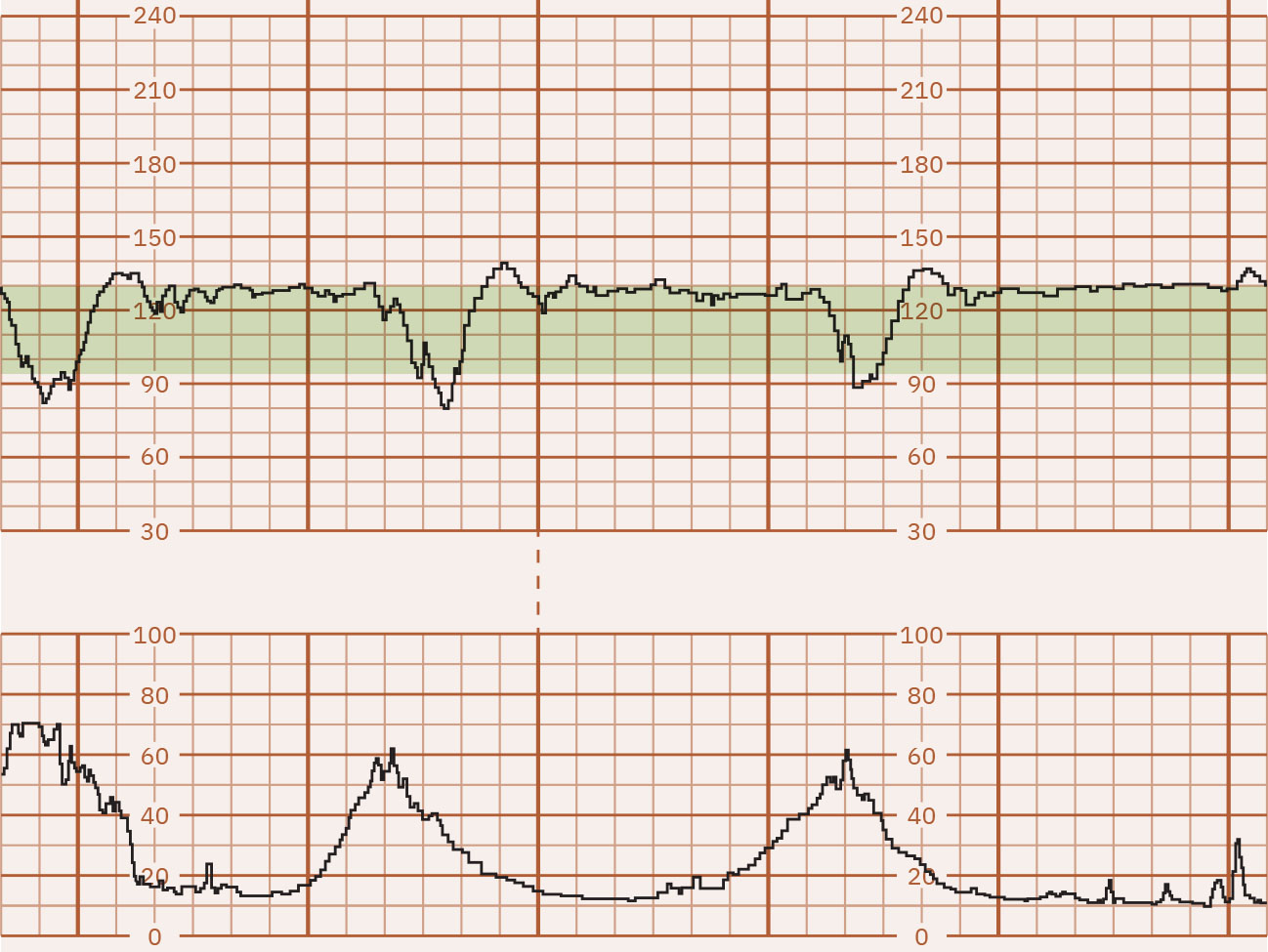 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
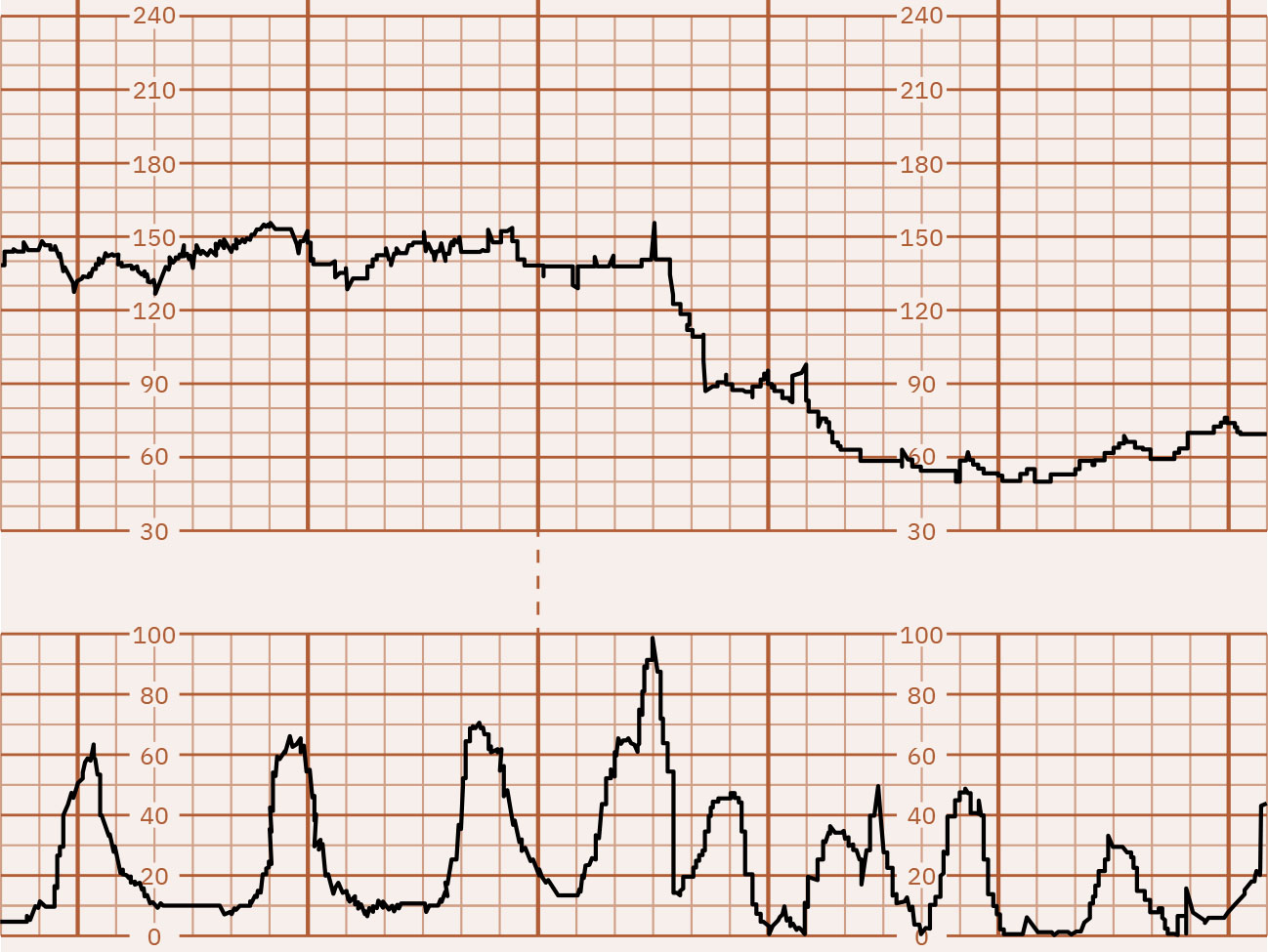 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.1.
- Contraction pattern: Adequate labor activity is generally 5 or fewer contractions in 10 minutes; tachysystole is more than 5 in 10 minutes across at least two intervals or contractions lasting 2 minutes or longer.
- NICHD category system: Category I is reassuring, Category II is indeterminate, and Category III is abnormal with highest acidemia risk.
Nursing Assessment
NCLEX Focus
Priority assessment asks whether current tracing suggests reassuring adaptation or evolving fetal hypoxia that needs immediate intrauterine resuscitation.
- Determine baseline and identify tachycardia (>160 for 10 minutes) or bradycardia (<110 for 10 minutes).
- When tachycardia is present, screen reversible maternal contributors first (especially fever) and avoid labeling fetal distress from baseline rate alone when decelerations and other compromise cues are absent.
- For baseline tachycardia, review maternal (infection/fever, anxiety, dehydration, nicotine, selected medications, thyroid context) and fetal (hypoxia, infection, anemia, prematurity, arrhythmia) contributors.
- For baseline bradycardia, review maternal (hypotension/anesthesia effect, metabolic causes, selected medications, major obstetric emergencies, and possible maternal-pulse misread) and fetal (head/cord compression, hypoxia, congenital conduction issues) contributors.
- Classify variability, emphasizing loss of moderate variability as a key warning trend.
- For minimal variability, check common contributors such as fetal sleep cycles, prematurity, CNS anomaly context, and medication exposure (including magnesium sulfate) before assigning irreversible compromise.
- Escalate promptly when variability trajectory worsens (moderate to minimal to absent), because this progression can signal advancing fetal stress.
- Differentiate deceleration type by onset, shape, relation to contractions, and recovery timing.
- Treat recurrent late decelerations as nonreassuring until proven otherwise, and evaluate likely uteroplacental-insufficiency drivers (tachysystole, oxytocin effect, neuraxial hypotension, hypertensive/placental disease, anemia contexts).
- Evaluate contraction frequency/duration/intensity and identify tachysystole patterns that worsen fetal tolerance.
- For variable decelerations, trend depth/frequency/duration and whether they are repetitive over time because prolonged repetition increases hypoxia concern.
- For prolonged decelerations, investigate hyperstimulation, cord compression, hypotension, abruption, seizure, and impending birth; deeper/longer episodes raise hypoxia risk.
- After prolonged deceleration recovery, treat persistent tachycardia with reduced variability as possible posthypoxic stress signal.
- Interpret the tracing as Category I, II, or III and trend whether the category is improving or worsening after interventions.
Nursing Interventions
- Reposition laboring patient, initiate IV fluid bolus when indicated, and escalate nonreassuring changes to provider promptly.
- For bradycardia concern, prioritize rapid differentiation between sustained baseline bradycardia and prolonged deceleration while beginning immediate repositioning and IV fluid support sequence.
- For concerning bradycardia or deceleration patterns, implement unit intrauterine resuscitation sequence and continuous reassessment.
- Stop oxytocin when uterine tachysystole contributes to nonreassuring FHR changes and prepare for tocolysis when ordered.
- Communicate pattern evolution clearly using standardized terminology to support team decisions.
Hypoxia Escalation
Persistent late decelerations, prolonged decelerations, or progressive variability loss can indicate worsening fetal oxygen compromise and require urgent action.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| tocolytics | Terbutaline use context | May be used when tachysystole contributes to fetal bradycardia; verify maternal pulse before administration. |
| labor-analgesics | Epidural and other options | Interpret tracing changes with medication effects and maternal status in mind. |
Clinical Judgment Application
Clinical Scenario
A laboring patient develops repetitive variable decelerations followed by a prolonged deceleration after frequent contractions.
- Recognize Cues: Abrupt recurrent decelerations, prolonged nadir, and contraction stress pattern.
- Analyze Cues: Umbilical cord compression with possible emerging fetal hypoxia.
- Prioritize Hypotheses: Immediate fetal oxygenation risk is highest priority.
- Generate Solutions: Reposition, fluid support, evaluate contraction burden, and notify provider urgently.
- Take Action: Start intrauterine resuscitation measures and maintain close tracing surveillance.
- Evaluate Outcomes: Baseline/variability improve and decelerations decrease in frequency or severity.
Related Concepts
- external-and-internal-fetal-monitoring - Monitoring method affects signal reliability and response speed.
- intrauterine-resuscitation - Escalation bundle for nonreassuring fetal status.
- stages-of-labor - Stage context informs expected tracing and contraction dynamics.
- physiologic-adaptations-during-labor-and-birth - Maternal adaptations influence fetal tracing interpretation.
- birth-related-complications - Core mechanism behind many variable deceleration patterns.
Self-Check
- Which FHR variability category is most reassuring and why?
- How do late decelerations differ from early decelerations in clinical significance?
- Which first nursing actions are prioritized for prolonged fetal bradycardia?