Interventions during Birth
Key Points
- Operative vaginal birth uses forceps or vacuum when expedited vaginal delivery is clinically indicated.
- In second-stage fetal compromise, expedited pathways can include episiotomy, operative vaginal delivery, or emergency cesarean escalation.
- Informed consent, preparation, and neonatal readiness are core nursing priorities.
- Nursing care must balance rapid intervention support with safety surveillance for parent and newborn.
Pathophysiology
Interventions during birth are used when spontaneous vaginal progress or fetal tolerance makes assisted delivery safer than continued unassisted pushing. Forceps and vacuum devices provide controlled traction to facilitate delivery during the second stage.
These interventions can reduce delay-related risk but introduce procedure-specific maternal and neonatal injury risks. Nursing assessment and preparation therefore focus on indication clarity, consent integrity, equipment readiness, and immediate post-delivery evaluation.
Classification
- Forceps-assisted birth: Instrument-guided traction applied to fetal head under defined criteria.
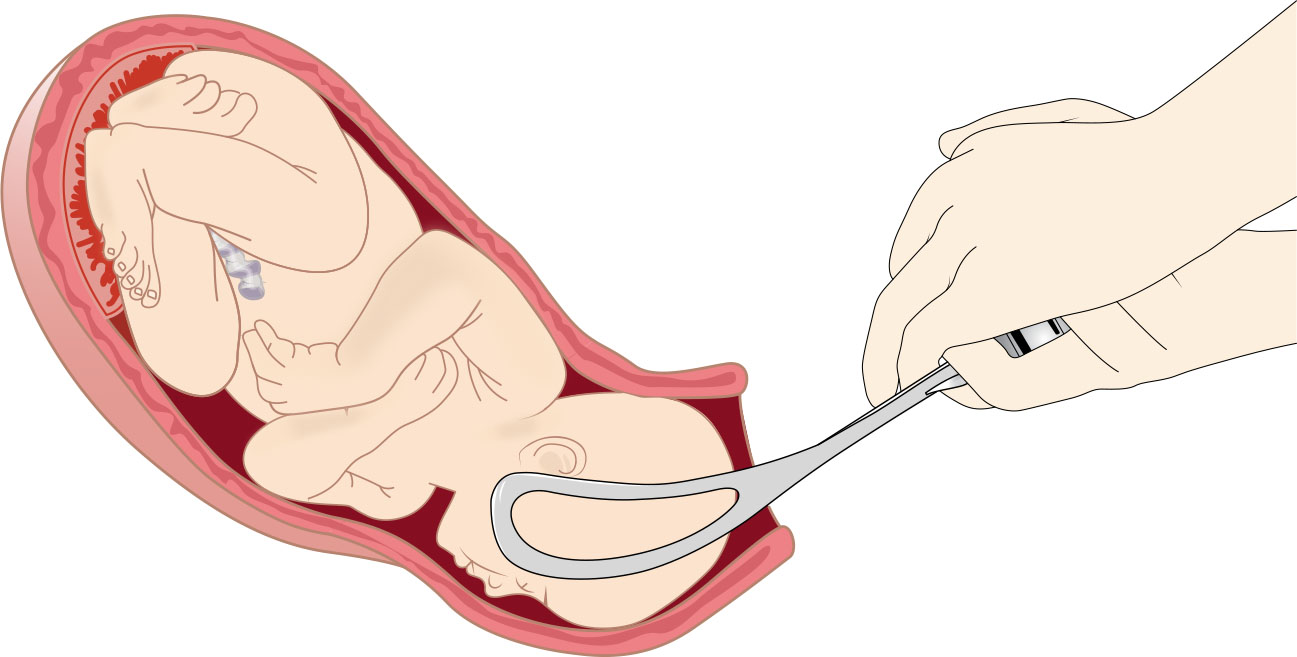 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.19.5.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.19.5.
- Vacuum-assisted birth: Cup-based traction synchronized with contractions and maternal effort.
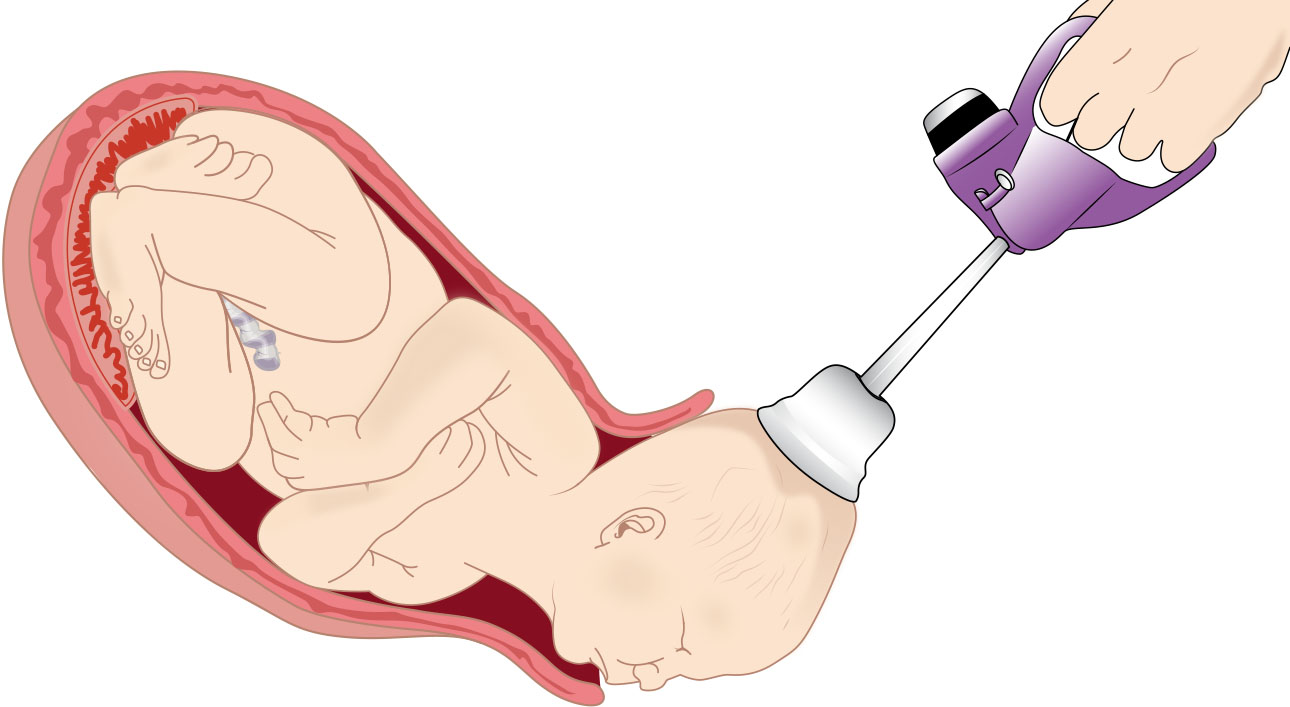 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.19.6.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.19.6.
- Episiotomy support context: Provider incision to enlarge the vaginal opening for selected urgent second-stage indications.
- Escalation pathway: Transition to cesarean delivery when operative vaginal criteria are unmet or unsuccessful.
Nursing Assessment
NCLEX Focus
Priority questions test pre-procedure readiness steps and the first response when assisted delivery criteria are not met.
- Verify indication, fetal status, station/position information, and provider readiness for operative approach.
- Treat persistent abnormal fetal tracing (for example late decelerations or bradycardia beyond 2 minutes) as high-priority cue for expedited birth planning.
- Confirm forceps prerequisites are met: full dilation, ruptured membranes, low fetal head, and no suspected cephalopelvic disproportion.
- Include forceps indication checks for maternal exhaustion, nonreassuring fetal status, prolonged second stage, and selected after-coming breech-head delivery.
- Confirm informed consent discussion was completed and patient understanding is documented.
- Treat operative vaginal birth consent as procedure-specific (not just routine admission consent): confirm indication, risks/benefits, and shared decision discussion occurred before attempt.
- Assess analgesia adequacy, bladder status, and maternal positioning before instrumentation.
- Screen for vacuum contraindications, including face/breech presentation, cephalopelvic disproportion, fetal head anomaly, preterm fetus, or known fetal bleeding risk.
- Ensure newborn support team presence due to higher immediate assessment/resuscitation risk.
Nursing Interventions
- Prepare lithotomy setup and procedural equipment while maintaining sterile field and patient privacy.
- Empty bladder, coordinate anesthesia support, and communicate procedure steps to patient/support person.
- When forceps is chosen, ensure lithotomy setup, bladder emptying, and epidural analgesia adequacy check before instrumentation.
- Monitor fetal heart rate and maternal response continuously through assisted-delivery attempts.
- During vacuum-assisted birth, support pressure cycling with contraction phases (increase suction during push/contraction, decrease between contractions) per provider workflow.
- For vacuum setup, assist stirrup positioning and confirm vacuum system integrity (including leak check) before traction attempts.
- For forceps delivery, monitor closely for maternal laceration/hematoma or urinary-tract injury and for neonatal facial/cranial injury cues.
- Recognize less common but high-severity forceps complications (maternal uterine rupture or trauma-related psychological distress, neonatal intracranial hemorrhage or seizure).
- For vacuum delivery, monitor newborn for scalp trauma, cephalohematoma, subgaleal hemorrhage, retinal hemorrhage, or intracranial injury signs.
- Assist rapid transition to cesarean pathway when operative attempts are contraindicated, unsuccessful, or fetal status worsens.
- Document indication, consent, timeline, outcomes, and any complications precisely.
- Document that consent conversation allowed questions and unbiased explanation of alternatives, benefits, and risks.
Failed or Unsafe Attempt Risk
Repeated or poorly indicated operative attempts increase maternal and neonatal harm and may require urgent cesarean transition.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| labor-analgesics | Regional/local analgesia context | Adequate pain control is required before operative traction attempts. |
| uterotonics | Post-birth management context | Frequently needed after delivery to support uterine tone and bleeding control. |
Clinical Judgment Application
Clinical Scenario
A prolonged second stage with increasing fetal stress prompts provider recommendation for operative vaginal birth.
- Recognize Cues: Delayed descent, fetal status concern, and need for expedited delivery.
- Analyze Cues: Assisted vaginal intervention may reduce delay-related risk if criteria are met.
- Prioritize Hypotheses: Immediate priority is safe preparation and informed, coordinated execution.
- Generate Solutions: Confirm consent/readiness criteria, optimize positioning and analgesia, and mobilize neonatal support.
- Take Action: Assist procedure while maintaining real-time monitoring and communication.
- Evaluate Outcomes: Delivery is completed safely or escalated promptly if attempt is unsuccessful.
Related Concepts
- nursing-care-during-the-second-stage-of-labor - Assisted birth decisions arise from second-stage progression and tolerance data.
- labor-dystocia - Common pathway leading to operative intervention consideration.
- fetal-heart-rate-and-contraction-patterns - Tracing deterioration can drive need for expedited birth.
- preexisting-conditions-placing-delivery-at-risk - Comorbid risk can lower threshold for intervention.
- postpartum-hemorrhage - Post-intervention surveillance includes bleeding-risk management.
Self-Check
- Which readiness checks are mandatory before forceps or vacuum use?
- When should operative vaginal birth be abandoned for cesarean escalation?
- Which documentation elements are most critical after assisted delivery?