Stages of Labor
Pathophysiology
Labor proceeds through first stage (onset of true labor through full 10 cm dilation), second stage (expulsive stage through birth), third stage (placental delivery), and fourth stage (immediate 1 to 4 hour recovery). Progress depends on maternal-fetal physiology and care environment.
The first stage includes latent and active phases. Typical latent-phase duration may extend up to about 20 hours in nulliparous and up to about 14 hours in multiparous labor. Active labor is generally identified at 6 cm dilation, after which progress is expected to accelerate with stronger, closer contractions. Active-phase contractions are commonly every 2 to 5 minutes with roughly 60-second duration and increasing support needs. When active-phase dilation stops despite continued observation, arrest concerns rise (for example, no dilation change for about 4 hours with consistent contractions or about 6 hours without consistent contractions). Cervical landmarks across stages are commonly summarized as early first stage 0 to 6 cm, active first stage 6 to 10 cm, second stage 10 cm to birth, and third stage birth to placental delivery with progressive cervical closure.
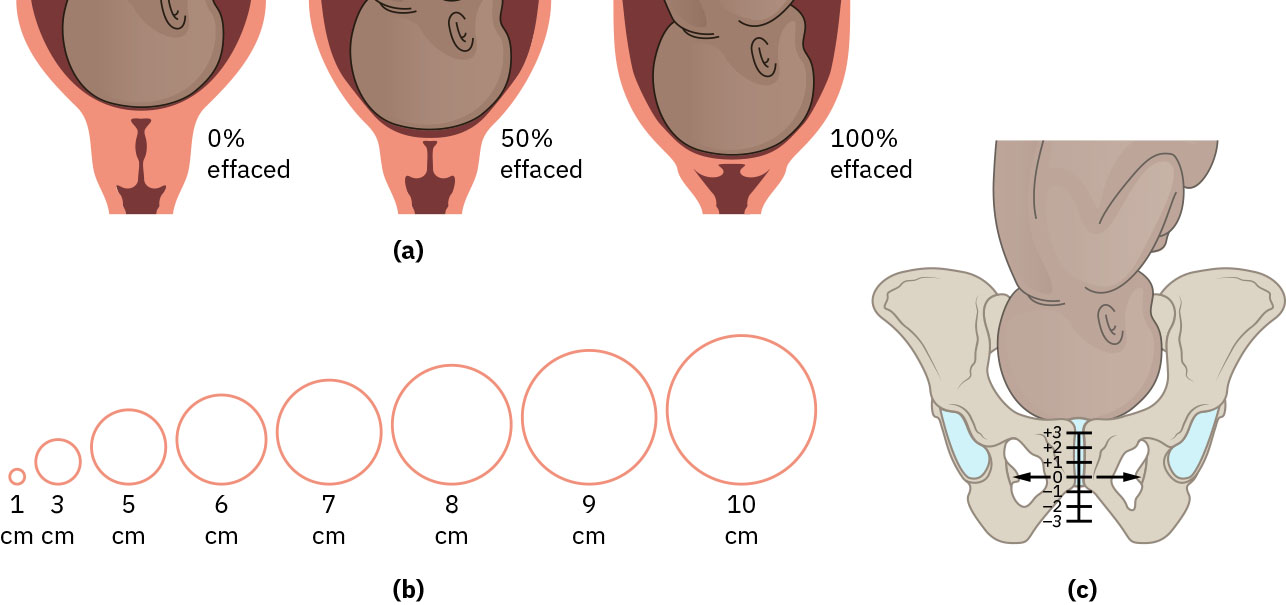 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.15.1.
Nursing Assessment
- Track dilation, effacement, station, and contraction pattern.
- Monitor maternal coping, fatigue, and fetal tolerance each stage.
- Assess placental separation signs and postpartum bleeding risk in third/fourth stages.
- Track stage-typical contraction patterns and duration trends (for example, first-stage latent vs active and second-stage strong 2-3 minute contraction spacing).
- In early labor triage, distinguish prodromal signs from true labor and assess rupture-of-membranes details (time, color, amount, odor).
- Use parity context when reviewing expected stage durations (for example, second stage commonly under 4 hours in first birth and under 3 hours in multiparous birth).
Nursing Interventions
- Match support strategies to stage and phase intensity.
- Use position changes and stage-appropriate coping guidance.
- Prepare for escalation when progression stalls or distress patterns emerge.
- Prioritize one-to-one surveillance in vulnerable immediate postpartum phase.
- Teach stage transition expectations and when to contact/return for care if contractions become regular/intensifying or concerning bleeding/fluid changes occur.
- During first-stage active-labor concern, escalate stalled cervical-change trajectories promptly to avoid delayed dystocia management.