External and Internal Fetal Monitoring
Key Points
- Intermittent auscultation with fetoscope or Doppler supports mobility but does not create a tracing record.
- Continuous external monitoring uses ultrasound and tocodynamometer to trend fetal heart rate and contraction frequency/duration, but toco does not directly quantify contraction intensity.
- Internal monitoring (FSE and IUPC) gives more precise data but requires cervical dilation and ruptured membranes and introduces additional risks.
- Monitoring choice depends on clinical need, signal quality, risk status, and patient mobility goals.
Pathophysiology
Intrapartum monitoring tracks fetal response to labor stress and uterine activity patterns to identify adaptation versus compromise. Reliable interpretation requires clear signal acquisition, stage context, and recognition of when additional monitoring precision is needed.
External methods are noninvasive and widely used but are vulnerable to signal loss with movement and cannot directly quantify contraction strength. Internal methods improve data precision, especially for contraction intensity and difficult tracings, but require invasive placement and carry infection and injury risk.
Intermittent auscultation is a third method that combines palpation of uterine activity with timed fetal heart auscultation before, during, and after contractions. It preserves ambulation and comfort options but lacks a continuous visual tracing history for team review and documentation.
Comparative-outcome data have shown mixed benefits of continuous electronic monitoring: seizure reduction in some neonatal cohorts without consistent reduction in overall fetal death or cerebral palsy, so method selection should stay risk- and goal-aligned.
Classification
- Intermittent auscultation: Fetoscope or Doppler spot assessment of FHR with concurrent palpation of uterine activity.
- IA interval guidance (example framework): Latent/active first stage often every 15 to 30 minutes, second-stage passive descent about every 15 minutes, and active pushing every 5 to 15 minutes (per policy/risk/provider order context).
- External FHR monitoring: Ultrasound transducer placed over fetal back.
- External UC monitoring: Tocodynamometer for frequency and duration trends.
- Internal FHR monitoring: Fetal scalp electrode (FSE) attached to fetal scalp.
- Internal UC monitoring: Intrauterine pressure catheter (IUPC) for contraction strength and resting tone in mm Hg.
Nursing Assessment
NCLEX Focus
Priority questions often ask when external monitoring is insufficient and internal monitoring should be considered or escalated.
- Perform Leopold maneuvers to optimize transducer placement and maintain trace quality.
- During intermittent auscultation, palpate contraction frequency/intensity/duration and auscultate fetal rate before, during, and after contractions to capture periodic change cues.
- When using Doppler for intermittent auscultation, compare maternal pulse to confirm fetal rather than maternal rate detection.
- Fetoscope detection is typically useful from about 20 weeks onward; Doppler can be used in antepartum visits and intrapartum care.
- Place auscultation device over the fetal back identified by Leopold maneuvers (commonly lower abdomen for vertex and above umbilicus for breech when heart sounds are loudest).
- Use structured Leopold sequence for placement confidence: fundal content, lateral/back location and lie, presenting part above pubis (C-grasp), and descent/flexion cues while facing maternal feet.
- During contraction palpation, compare intensity against practical tactile anchors (mild/cheek, moderate/nose-tip, strong/forehead firmness) alongside patient report.
- For low-risk intermittent monitoring plans, reassess FHR at interval frequencies commonly ranging from every 15 to 60 minutes, increasing with risk status and labor progression.
- For first-stage electronic monitoring, a common cadence framework is: less than 4 cm by provider discretion; 4 to 5 cm every 30 minutes if low risk and every 15 minutes with risk factors or oxytocin; 6 cm or greater every 30 minutes if low risk and every 15 minutes with risk factors or oxytocin.
- When continuous monitoring is used, document FHR/UC interpretation at least every 15 to 30 minutes with a brief fetal-status summary.
- Assess for signal quality loss with maternal/fetal movement and reposition devices promptly.
- Teach that external signal dropouts can occur with maternal/fetal movement and instruct patient to call for prompt transducer readjustment rather than assuming emergency.
- Identify prerequisites for internal monitoring, including membrane rupture, cervical dilation, and ability to palpate presenting part for safe placement.
- If membranes remain intact but internal data are needed, escalate for provider-level risk-benefit decision on amniotomy before placement attempts.
- Monitor for internal-monitor complications such as infection, bleeding, uterine/placental injury risk, and fetal scalp concerns.
- Recognize common internal-monitor escalation contexts: nonreassuring FHR, low amniotic fluid context, persistent external signal loss, and uterotonic induction/augmentation requiring precise contraction quantification.
- Interpret contraction pattern using standardized terms: frequency (start-to-start), duration (start-to-end), and strength (palpation grade externally or mm Hg with IUPC).
- On standard strip display, recognize top FHR tracing, bottom uterine-contraction tracing, and midline maternal pulse trace to reduce misread risk.
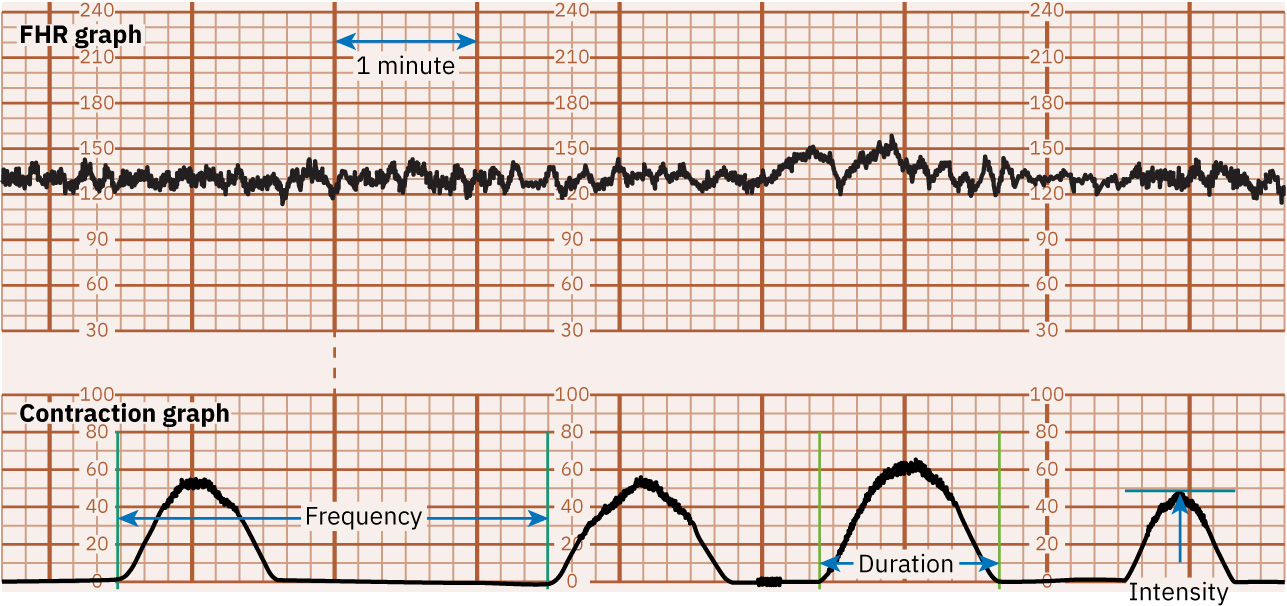 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.16.2.
- Use expected uterine-activity ranges as reference (commonly 5 or fewer contractions in 10 minutes with duration about 45 to 60 seconds, sometimes up to about 90 seconds near second stage).
- Diagnose tachysystole by frequency burden or prolonged-length criteria (for example more than 5 contractions in 10 minutes or contraction length around 2 minutes or longer within a 30-minute window).
- Calculate Montevideo units only with IUPC by summing each contraction peak minus resting tone over a 10-minute period.
Nursing Interventions
- Apply and secure external monitors appropriately while preserving mobility when feasible.
- Place ultrasound transducer over fetal back near the fetal head (not directly over fetal chest/extremity-dense zones), use acoustic gel, and secure with belt/adhesive per device.
- Place toco over the firmest fundal area (often over fetal buttocks in cephalic presentation) and adjust to optimize contraction-frequency/duration capture.
- Educate the patient on available monitoring-method options and rationale at each stage/risk context to support informed shared decision-making.
- Explain IA tradeoffs explicitly: improved mobility and comfort versus higher one-to-one staffing demand and lack of continuous strip archive for team review.
- For continuous external monitoring, place ultrasound and toco devices with belts/adhesives and select wireless/water-compatible systems when available to preserve movement or hydrotherapy goals.
- Escalate toward continuous monitoring when high-risk contexts are present (for example meconium-stained fluid, multiple gestation, preeclampsia, neuraxial anesthesia, or dysfunctional labor trajectory).
- Explain external-monitor tradeoffs: easier setup and centralized multi-room tracing review/documentation versus potential mobility limits and recurrent signal dropouts with movement.
- Note that external monitoring can be used regardless of membrane status or cervical dilation, while internal monitoring requires ruptured membranes and invasive placement conditions.
- During FSE placement support, avoid fontanelle regions per operator guidance and maintain sterile workflow.
- Explain internal-monitor tradeoffs clearly: greater precision for deceleration timing/variability and quantified uterine pressure versus higher infection/injury risk from invasive placement.
- Escalate to provider for internal monitor placement when tracing quality or risk profile warrants deeper surveillance.
- Ensure internal monitor insertion is performed by trained personnel using sterile technique after confirming dilation and membrane prerequisites.
- For FSE support, confirm presenting head is low/palpable and cervix permits insertion; identify sutures/fontanelles first, avoid fontanelle placement, and secure electrode per operator technique before trace validation.
- For IUPC support, verify depth markers during insertion to reduce perforation risk and escalate immediately if frank red blood appears during introducer advancement.
- Use IUPC data to evaluate contraction adequacy and support oxytocin-related decisions.
- For tachysystole with nonreassuring FHR, initiate immediate bundle: discontinue oxytocin, lateral repositioning, IV bolus (commonly 500 mL LR if not contraindicated), oxygen by mask 8-10 L/min, and prepare/assist with terbutaline 0.25 mg SQ per order.
- For tachysystole with reassuring FHR, reposition laterally and give IV bolus; if unresolved after about 10 minutes reduce oxytocin by half, and if still unresolved after another 10 minutes stop oxytocin until activity returns to 5 or fewer contractions in 10 minutes.
- Notify provider early during tachysystole management and keep terbutaline readily available; if tachysystole resolves within about 30 minutes, oxytocin restart is typically at half of the prior rate per protocol/order.
- When oxytocin is being titrated, document fetal status before and after each dose increase.
- Document standardized interpretation sequence: monitoring method (external/internal), baseline rate and variability, accelerations/decelerations with type, contraction frequency-duration-intensity and resting tone status, category (I/II/III), and care plan with communication/new orders.
Internal Monitoring Risks
Internal devices improve precision but increase infection and procedural injury risk; strict indication and sterile technique are essential.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| uterotonics | Oxytocin augmentation context | IUPC can help quantify contraction response and guide safe titration. |
| labor-analgesics | Epidural/spinal context | Monitoring intensity may need adjustment in higher-risk or anesthetized labor. |
Clinical Judgment Application
Clinical Scenario
A laboring patient with epidural anesthesia has recurrent signal loss on external tracing and evolving nonreassuring pattern concern.
- Recognize Cues: Intermittent external signal loss and uncertain FHR interpretation.
- Analyze Cues: Current monitoring may be insufficient for safe real-time decision-making.
- Prioritize Hypotheses: Priority is obtaining reliable fetal and contraction data quickly.
- Generate Solutions: Reposition external devices, reassess Leopold findings, and request internal monitoring if unresolved.
- Take Action: Implement escalation pathway and continue close bedside surveillance.
- Evaluate Outcomes: Stable high-quality tracing supports accurate interpretation and intervention timing.
Related Concepts
- fetal-heart-rate-and-contraction-patterns - Core terminology is required before monitor interpretation.
- physiological-influences-on-fetal-heart-rate-patterns - Etiology guides response to abnormal tracings.
- intrauterine-resuscitation - Nonreassuring findings trigger immediate corrective actions.
- stages-of-labor - Stage influences expected contraction and tracing dynamics.
- oxytocin-therapy - Contraction monitoring quality is critical during augmentation.
Self-Check
- What are the key limitations of the external tocodynamometer compared with IUPC?
- Which prerequisites must be present before internal monitor placement?
- Which tracing-documentation sequence best supports rapid team interpretation?