Anesthesia for Labor and Birth
Key Points
- Epidural anesthesia is common in labor and requires structured pre-, intra-, and post-insertion nursing surveillance.
- Spinal and general anesthesia provide rapid surgical anesthesia, but each has distinct maternal and neonatal risks.
- Nursing priorities center on hemodynamic stability, fetal perfusion, airway and aspiration safety, and informed patient education.
Pathophysiology
Obstetric anesthesia modifies neural transmission to reduce pain and facilitate vaginal or surgical birth. Regional techniques (epidural, spinal, pudendal, local infiltration) target specific pathways, while general anesthesia induces systemic unconsciousness. The physiologic challenge is to provide sufficient analgesia or anesthesia without compromising maternal circulation, ventilation, placental perfusion, or neonatal transition.
Epidural-related sympathetic blockade can decrease vascular tone and trigger maternal hypotension, which may reduce uteroplacental perfusion and produce fetal late decelerations or bradycardia. Less common epidural complications include maternal bradycardia, respiratory depression, infection, paresthesia, and rare nerve injury. General anesthesia agents cross the placenta and may depress neonatal respiration, making delivery timing and immediate newborn support critical. Spinal anesthesia has near-immediate onset and complete sensory and motor block, while local infiltration or pudendal blockade provides focused perineal anesthesia with preserved consciousness and limited systemic effects.
Classification
- Epidural anesthesia: Continuous regional infusion in epidural space, commonly T10 to S5 coverage in labor, often with patient-controlled bolus capability.
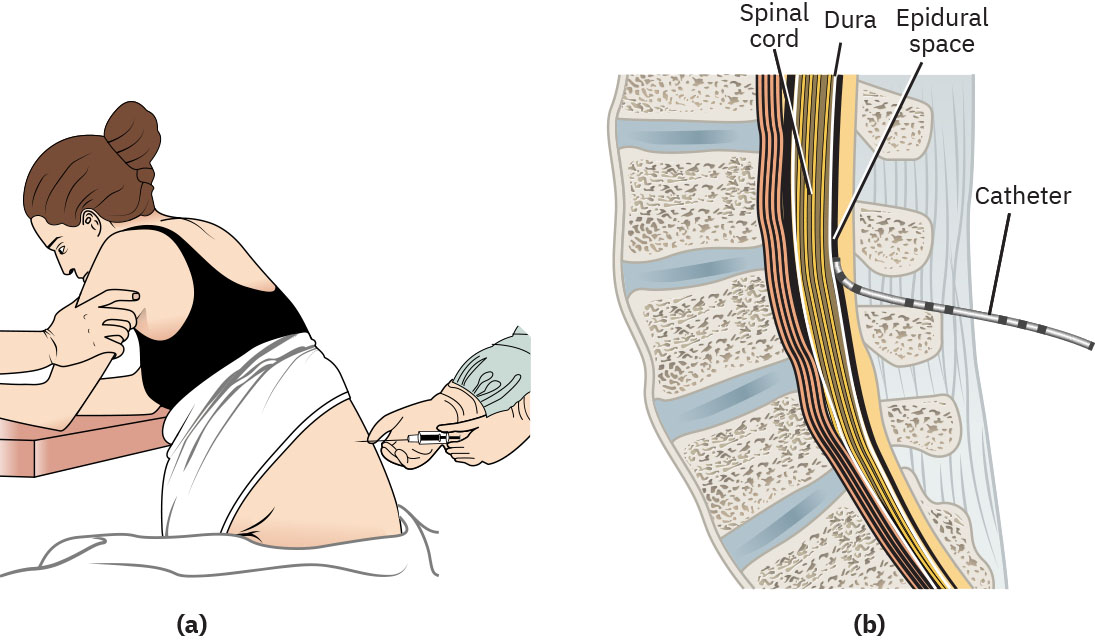 Illustration reference: OpenStax Maternal-Newborn Nursing Ch.17.3.
Illustration reference: OpenStax Maternal-Newborn Nursing Ch.17.3.
- Pudendal block/local infiltration: Perineal-focused anesthesia for operative vaginal birth or advanced laceration repair with limited maternal sedation and preserved motor function.
- Spinal block: Single-dose intrathecal anesthesia with rapid onset, often for cesarean birth.
- General anesthesia: Systemic unconscious anesthesia for urgent or contraindicated regional-anesthesia scenarios.
Nursing Assessment
NCLEX Focus
Priority items include contraindication screening, post-placement hypotension recognition, and fetal response monitoring during maternal hemodynamic changes.
- Verify informed consent, review eligibility criteria, and report critical labs such as platelet count before epidural placement.
- Identify contraindications including coagulopathy, hypovolemia, thrombocytopenia, infection, severe valvular disease, or severe left ventricular outflow obstruction.
- Include neurologic disease and local-anesthetic allergy in epidural contraindication screening.
- Establish baseline maternal-fetal status with continuous blood pressure, pulse oximetry, and fetal monitoring before regional anesthesia.
- Anticipate technically difficult epidural placement in obesity; anesthesia providers may require longer-needle equipment.
- For general anesthesia candidates, screen for aspiration and difficult-airway risk and anticipate higher failed-intubation risk in pregnancy-related airway edema/anatomic change.
- Reassess frequently after placement for hypotension, respiratory depression, neurologic symptoms, urinary retention, and adequacy of pain control.
- Reassess whether anesthesia choice remains aligned with current labor stage/timing and patient preference as labor progresses.
Nursing Interventions
- Prepare for epidural insertion with IV fluid preload, positioning support, sterile-field assistance, and continuous monitoring.
- Support C-position setup for insertion, observe test-dose response, and document insertion timing and immediate adverse effects.
- During test dose, monitor and report red flags such as metallic taste, new difficulty speaking, sudden-onset headache, or neck pain.
- During and after insertion, document test-dose reactions, monitor blood pressure at required intervals (for example every 5 minutes in the first 30 minutes, then every 15 minutes per protocol), and escalate hypotension management promptly.
- Implement fall precautions and mobility restrictions after regional anesthesia; manage bladder care with intermittent or indwelling catheterization per labor stage and remove indwelling catheters before active pushing in second stage.
- After insertion, position with lateral tilt or wedge support to reduce aortocaval compression risk and preserve perfusion.
- If fluid bolus is ineffective or contraindicated during postepidural hypotension, anticipate provider-directed vasopressor support (for example ephedrine).
- If intrapartum cesarean becomes necessary, anticipate dosing the existing labor epidural to deeper surgical anesthesia when appropriate.
- For spinal anesthesia, anticipate complete motor/sensory loss after single intrathecal dosing and reinforce transfer/position safety until block regression.
- Prepare local anesthesia/pudendal procedures for episiotomy or laceration repair by organizing sterile supplies and counseling about infiltration sting and possible incomplete relief.
- Teach advantages, limits, and side effects of epidural, pudendal, local, spinal, and general anesthesia so patients can make stage-appropriate decisions.
- For general anesthesia cases, support aspiration-prevention and airway workflows, then prioritize rapid maternal-neonatal assessment after delivery.
- During emergency general anesthesia, support rapid-delivery workflow, assist with airway-safety steps (including cricoid-pressure role per policy/training), and prepare for neonatal respiratory support and lower-Apgar risk.
Postepidural Hypotension Risk
Persistent hypotension can reduce uteroplacental perfusion and worsen fetal status; rapid fluids, provider notification, and ordered vasopressor support are time-critical.
Epidural analgesia can fail technically (malposition, migration, incomplete block). Maintain backup pain pathways, reassess symmetry/coverage, and re-escalate to anesthesia promptly when relief is inadequate.
Pharmacology
| Drug Class | Examples | Key Nursing Considerations |
|---|---|---|
| Anesthesia For Labor And Birth (local-anesthetics) | Bupivacaine, lidocaine | Monitor for hypotension, neurologic/cardiac toxicity signs, and block adequacy. |
| opioids (opioid-analgesics) | Fentanyl, intrathecal morphine | Evaluate respiratory status and sedation, and coordinate postpartum monitoring. |
| vasopressors | Ephedrine context | Used for significant postepidural hypotension when fluid response is insufficient. |
| hypersensitivity-types-and-anaphylaxis-response (antiemetics-and-antihistamines) | Nausea/itching treatment context | Support comfort and safety after neuraxial dosing. |
Clinical Judgment Application
Clinical Scenario
A laboring patient receives a new epidural and develops blood pressure decline with emerging fetal late decelerations.
- Recognize Cues: Maternal hypotension, recent epidural dosing, and fetal perfusion-sensitive tracing changes.
- Analyze Cues: Sympathetic blockade is likely reducing uteroplacental blood flow.
- Prioritize Hypotheses: Immediate risk is progressive fetal compromise if maternal perfusion is not restored.
- Generate Solutions: Increase IV fluids, optimize position, notify anesthesia/obstetric team, and prepare ordered vasopressor therapy.
- Take Action: Implement corrective measures and continuous maternal-fetal reassessment.
- Evaluate Outcomes: Maternal pressure stabilizes and fetal tracing improves, allowing safe continuation of labor.
Related Concepts
- pharmacological-pain-management - Medication-based analgesia often precedes or complements anesthesia decisions.
- nonpharmacological-pain-management - Nonpharmacologic methods remain useful adjuncts after regional placement.
- external-and-internal-fetal-monitoring - Reliable monitoring is required to detect fetal effects of maternal hemodynamic change.
- fhr-and-uc-intervention-framework - Provides escalation pathways when tracing abnormalities emerge.
- intrauterine-resuscitation - May be required when fetal compromise persists despite maternal stabilization efforts.
Self-Check
- Which findings make a laboring patient a poor candidate for epidural anesthesia?
- What are the highest-priority nursing actions when postepidural hypotension occurs?
- Why is general anesthesia used less frequently in childbirth despite immediate onset?